Also known as prior level of function in case you aren’t in to abbreviations. How many times have you written that today? This week? This month? How much thought have you given to what PLOF actually looks like for that patient? Isn’t their PLOF why you are seeing them in the first place? Let’s unpack this…
This past year I have been writing, revising, and editing a chapter for a textbook specific to geriatric considerations in rehabilitation. I was working from an old edition and the phrase “prior level of function” kept showing up. Under every heading, we talked about returning a patient to their prior level of function. Proximal humerous fracture? Return to prior level of function. Vertebral compression fracture? Return to prior level of function. Spinal fusion? Return to prior level of function. But why?
I kept thinking, “Why would I want to return a patient to their prior level of function when that level of function is what lead them to this problem in the first place?” So it was time to change. Instead, I wrote about utilizing proper exercise prescription to rehabilitate a patient to a safe and healthy level of function to prevent further onset of acute medical events or progression of chronic ones. So what does a safe and healthy level of function look like? That’s the tricky part.
Time is the key factor. Setting the time frame of what the “prior level of function” was seems to be an issue of great debate in our profession. The answer to this question isn’t as hard as it seems. When was the patient last not experiencing any medical issues? That would be the prior level of function I would want to target with therapy. I realize that this could have been many years ago, but who is to say that they can’t recover? If they are determined enough and goal-driven, then why not try to get them there?
Why can’t my 85 year old patient with 6 weeks of ICU time for sepsis on 6L of oxygen and a 4pt walker rehab to his prior level of function without oxygen or a device?
Why can’t my patient with a C5 spinal cord injury from cliff diving walk with a cane a year after injury?
Why can’t my patient with COPD return to playing tennis?
Why can’t my patient with a partial knee replacement go back to running 5Ks in 3 weeks? Why can’t my patient with metastatic lung cancer on high flow oxygen climb up and down her stairs without desaturating?
If you are listing answers to these questions, like different impairments and limitations, you are really just listing your targets for intervention.
There is plenty of research out there on hip fracture outcomes. Most of this research says that if someone has a fall with a hip fracture, they can really only hope to rehab to one functional level lower than their prior level of function. We need to be thinking about this critically. Is this outcome a limitation of the patient potential? Is this outcome a limitation of the coverage availability? Or is this outcome a limitation of the clinician’s interventions? Maybe this outcome is, itself, creating a limitation on all of these things: the payer’s willingness to pay, the patient’s beliefs in their abilities, and the clinician’s inherent bias toward the patient’s potential. If we can only control what we can control, I’m going to choose to control my role in this scenario.
If a patient has a fall, starts using a walker for a few months, then falls again and ends up with a femoral neck fracture, gets a pinning, goes to rehab, and comes home with a new walker, why do I want her long term goals to be centered around walking safely with the walker? Of course, we have to take in to consideration the healing times frame of boney tissue, but we need to be looking long term. This patient’s prior level of function is not using a walker, it’s whatever their function was before they experienced the decline. And the interventions shouldn’t be only targeting her hip. She got that fracture from a fall so let’s also be working on her balance and gait speed and working toward getting her off the walker!
That patient with sepsis I mentioned above? He was back to fishing and yard work without oxygen and without a device in 8 weeks. That patient with COPD is back to playing tennis. That patient with the C5 cord injury walks with a cane still today. The patient with lung cancer not only climbed her stairs but also walked outside all the way around her home without desaturating. That patient with a partial knee replacement ran his 5K after 3 weeks (against my advice, and yes, he paid for it but he did it. He eventually recovered and was just fine. I was really doubtful on this one but patients can be very driven toward their goals!).
Don’t be the limiting factor in your patient’s recovery by choosing their prior level of function for them. Many people were on the slow decline prior to that event and haven’t been their normal selves in a while. Let their goals guide your understanding of the prior level of function they really want to return to. We are the ones who have the skills to get them back to the lives they want. Mary McMillan saw the future of physical therapists as the purveyors of hope. After all these years, we have the tools to turn hope into reality.
Was there ever a patient who achieved tremendous goals with you? Tell me your story in the comments!
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease
Did you know that PPE is actually the very last level of infection control??? To be honest, I have to admit that I had NO IDEA. Until COVID-19 became the impetus for my increase in research and writing, I had no idea that people other than healthcare professionals and their governing bodies were making an effort to reduce infection. And, I’m not commenting on everyone washing their hands or our sterilization teams (whom I consider to be in the group of healthcare professionals). I mean there are construction workers, HVAC people, contractors, architects, builders, and entire governing bodies that don’t work in patient care that do 85% of the work of infection control. Let’s call them out!
The infection control process is actually best illustrated as an upside down pyramid. Once you read through it, you will say to yourself, “Well, of course! I knew that!” But you didn’t really think of it until now, did you? There is actually an entire initiative dedicated to Prevention through Design! If you take a look at how this pyramid is constructed, you can see the levels of effectiveness are right alongside the intervention. And guess what? PPE is the LEAST effective method of infection prevention for patients and for healthcare workers. There is a link on the Resources page that will take you to the NIOSH document for infection prevention controls for more details about how some of these things are done.
I’m going to go through each of these steps to explain and give you an example of how this works. I’m going to use the hazard of stairs as my primary example. Obviously not an infection but may of these steps can’t apply to infection, which is why we need so many steps! But, they can all apply to stairs. Then we will go back and talk about infection control.
Elimination. If only it were this easy, right? Let’s just eliminate the hazard and then we don’t have to deal with it anymore. We all know it is never actually that easy. The flu can’t be eliminated so matter what we try. But there are some instances where elimination can work. Eliminate stairs from a hospital and you don’t have to worry about anyone falling down them. Keep everything on one level and no problems from stairs will arise. Obviously this can’t always be done, especially if the building has already been built, and we are trying to reduce the falls down the stairs 10 years later. That’s why there is another step…
Substitution. So instead of stairs, we can have elevators! Of course this isn’t a full substitution because we still have to have stairs in case of power outages, fires, and other emergencies. But if we substitute the major method of traversing floors in a facility to something safer than stairs, we can reduce the hazards that stairs pose. In the therapy world, this isn’t very functional because we know people use stairs at home and in the community. So let’s substitute actual flights of stairs with wooden framed in steps with handle bars on both sides. That will allow patients who need to perform stairs to practice them in a safe environment and reduce the hazard risk.
Engineering Controls. Ok, so let’s go back to the point of the hospital already being built and there are stairs. Can’t get rid of them. No problem. Engineering can come in and add controls. These types of things include hand rails, vertical bars on the turning platforms, gripper tape to the surfaces, yellow striped hazard tape to the edges of the steps, doors to the stairwell, and badge-locks to the doors. All of these things can help prevent the stairs from being as much of a hazard. There are many examples of engineering controls that apply to infection control, too, and we will investigate those later.
Administrative Controls. Policy policy policy. Change the policies, change the hazard risk. If it is policy that no one allows a patient on the stairs without supervision and assistance, odds decrease that the patient will get hurt. You can start to really see by now how these levels becomes less effective as we move down the pyramid.
PPE. For the sake of our stairs example, we are going to call a gait belt PPE. If we are going to use the stairs with someone who is unsafe and be there to provide them support, we can use equipment to decrease the risk of the training we are providing. However, placing the patient actually on the stairs for training is also the behavior that puts them at the highest risk of being injured. But we have to do it, right? So we use the gait belt to give ourselves a hand. It is our personal piece of equipment that helps (a bit) to prevent a hazard.
So how does all of this apply to viruses? Physical hazards are much easier to remove from the situation, but viruses can’t be fully removed. And substituting a different, less dangerous virus isn’t really a better option, nor is it feasible. So we have to come down to environmental controls next. Negative pressure isolation rooms are the most common thing we probably think of when it comes to treating patients who have a contagious condition. They are used for patients who have measles, influenza, and tuberculosis. The negative pressure room keeps all the air breathed in that room away from other rooms. The air is exchanged out individually, not entering the general air supply in the facility.
Speaking of the air supply, again, we are going to get a bit science-y here and talk about some fluid dynamics. Did you know that HVAC systems for hospitals actually have settings that allow for increased or decreased air exchange based on the square footage of the space and the concentration of people in it at any given time? Some can be self-altering based on occupancy, and some are static and have to be manually changed. A recent study was released that measured the air flow necessary to clear certain sized rooms with certain occupancy that would be required to reduce the transmission probability specific to COVID-19. They actually have it measured out how many cubic meters per minute of air they have to move so that no one would have to wait between using the bathroom for the air to be cleared (that’s 10 m3/min or 200 CFM (cubic feet per minute) for a single occupancy bathroom). For shared common spaces, the airflow needs to be 50 m3/min (or 2000 CFM) if the occupancy is fixed. If you are utilizing a public bathroom with several people in and out, the risk of transmission is difficult to control with this tool. Even air circulation patterns alter infection transmission which really comes in to play in oddly shaped spaces. If you are eating in a restaurant tucked away in that romantic corner, you are going to be more likely to transmit and/or receive transmission of infection due to lack of ventilation of aerosolized particles that are delivered to the space via “leaks” from the primary circulation of air in the restaurant.
While reading this article, I was thinking to myself, “So what is likely the highest risk thing or place right now based on these factors?” And the article didn’t disappoint. A choir practice in Seattle was studied as an epicenter of outbreak. The airflow in the small church was 20 m3/min and the choir had 60 members present for a 2.5 hour practice. The result of this practice was that 87% of the attendees became infected with COVID-19 from a single source. The authors discussed that choir practice significantly increased the rate of aerosolization with singing (this wasn’t the only choir outbreak) and that other activities such as indoor dance practices and working in a call center would be similar in transmission rate even IF hand hygiene and social distancing were utilized properly.
All of this to really demonstrate that Engineering controls can be put in place to prevent or decrease risk of transmission, but they have to be used properly. And if they are not, other measures put in place like hand washing and social distancing (both environmental controls as they try to remove the contagion) have little effect.
Why am I harping on about engineering controls? Why am I becoming concerned about the amount of air my HVAC system can move? This is why. New findings from this study include
1 min of loud speaking generates at least 1,000 virion-containing droplet nuclei that remain airborne for more than 8 min
the smallest droplet nuclei effectively remain airborne indefinitely and have half-lives that are dominated by the ventilation rate, at a saliva viral load of 7 × 106 copies per milliliter
Some patients have viral titers that exceed the average titer of Wölfel et al by more than two orders of magnitude thereby increasing the number of virions in the emitted droplets to well over 100,000 per minute of speaking.
The droplet nuclei observed in this present study and in previous studies are sufficiently small to reach the lower respiratory tract, which is associated with an increased adverse disease outcome
In essence, talking is sufficient to aerosolize COVID-19 particles and these particles remain in the air for at least 8 minutes. Then pair that with this study with these findings:
airborne transmission, particularly via nascent aerosols from human atomization, is highly virulent and represents the dominant route for the transmission of this disease [COVID-19]
the importance of airborne transmission has not been considered in establishment of mitigation measures by government authorities
And my personal favorite: It is also important to emphasize that sound science should be effectively communicated to policy makers and should constitute the prime foundation in decision-making amid this pandemic.
All three of these studies referenced recommend personal use of face coverings/masks as the only way to effectively reduce viral transmission and their effectiveness if increased with the addition of other controls such as social distancing and hand hygiene. However, these other controls are not effective without the use of face coverings/masks. For how to make a homemade mask that might actually work, check out this post.
So even though PPE is literally the WORST at controlling infectious transmission, and even though it truly is the last line of defense against transmission, it will end up being the best bet we’ve got. We can’t always control the environment we are in. We can’t substitute a different pathogen that is less virulent. We can implement engineering controls in the facilities we utilize, but not in the community or outdoors. We can add administrative controls to reduce the risk of infections. But ultimately, with COVID-19 and other respiratory pathogens like Measles and Tuberculosis, it’s going to come down to the PPE. Especially in the rehab professions, where close contact and use of different speech techniques are regularly utilized across disciplines, we need to be taking precautions, educating ourselves, and keep each other safe.
Do you work in environmental infection control? How has COVID-19 changed your day-to-day? Tell me in the comments!
Dr. Rebekah Griffith, other wise known as The ED PT, interviewed Dr. B on all things patient care management and how PTs in the ED and Home Health PTs can work together to provide the best possible care for patients. We talked about the struggles we each face in managing complex patients and the roles…
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!
References
Evans, M. (2020). Avoiding COVID-19: Aerosol guidelines. Massachusetts Institute of Technology: Department of Physics. Published by medRxiv [ahead of print]. Retrieved from https://doi.org/10.1101/2020/05/21/20108894
Stadnytskyi, V., Bax, C. E., Bax, A., Anfinrud P. (2020). The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proceedings of the National Academy of Sciences. 117 (22) 11875-11877; DOI: 10.1073/pnas.2006874117
Zhang, R., Li, Y., Zhang, A. L., Wang, Y., Molina, M. J. (2020). Identifying airborne transmission as the dominant route for the spread of COVID-19. Proceedings of the National Academy of Sciences. 202009637; DOI: 10.1073/pnas.2009637117
I can’t even begin to tell you guys how much I love teaching people about lung function in the presence of disease (read: HUGE NERD). Teaching patients how to correct for dynamic hyperinflation is one of those things that I really love teaching.
If you remember from a few weeks ago, we talked about how to facilitate hyperinflation for those who suffer from restrictive lung diseases like COVID-19, pulmonary fibrosis, or who were recently extubated. But for people with obstructive disease, hyperflation is actually their biggest issue. Airways get obstructed and CO2 gets trapped in the lung. This takes up space and prevents usable oxygen from reaching the alveoli. So, for people with obstructive diseases like COPD, cystic fibrosis, and emphysema, we actually need to decrease and prevent hyperinflation to improve their function.
Dynamic hyperinflation is hyperinflation that keeps building on itself as they takes breaths. The end result is that the usable space for tidal volume becomes less and less and the patient gets short of breath. Take a look at this video a made for you. It’ll help you understand dynamic hyperinflation as well as a few techniques to correct for it! Enjoy!
(Brockway, K., 2020)
Utilizing these techniques before you get started with exercise is important for a couple reasons. You want the patient to have the most lung volume available for tidal exchange which means getting all the trapped CO2 out that you can. Also, you want to give them some time to practice these techniques. It can be very difficult to breathe this way as oxygen demand increases with activity or exercise so practice is important. In addition to practice, your patient will probably need lots of cueing to keep this up as they become more active.
However, if you can start them off on a good tidal volume, improve their V/Q matching at rest and with activity, and rehabilitate them back to even better than where they were before, you are really doing them the service they need. Make sure to keep monitoring their oxygen saturations with training as they may sink as they learn how to change their breathing. They have spent years trying to figure out how to get air in and you will probably be the first one trying to teach them how to get air out!
What are your favorite methods for getting the old air out and the new air in? Tell me about them in the comments!
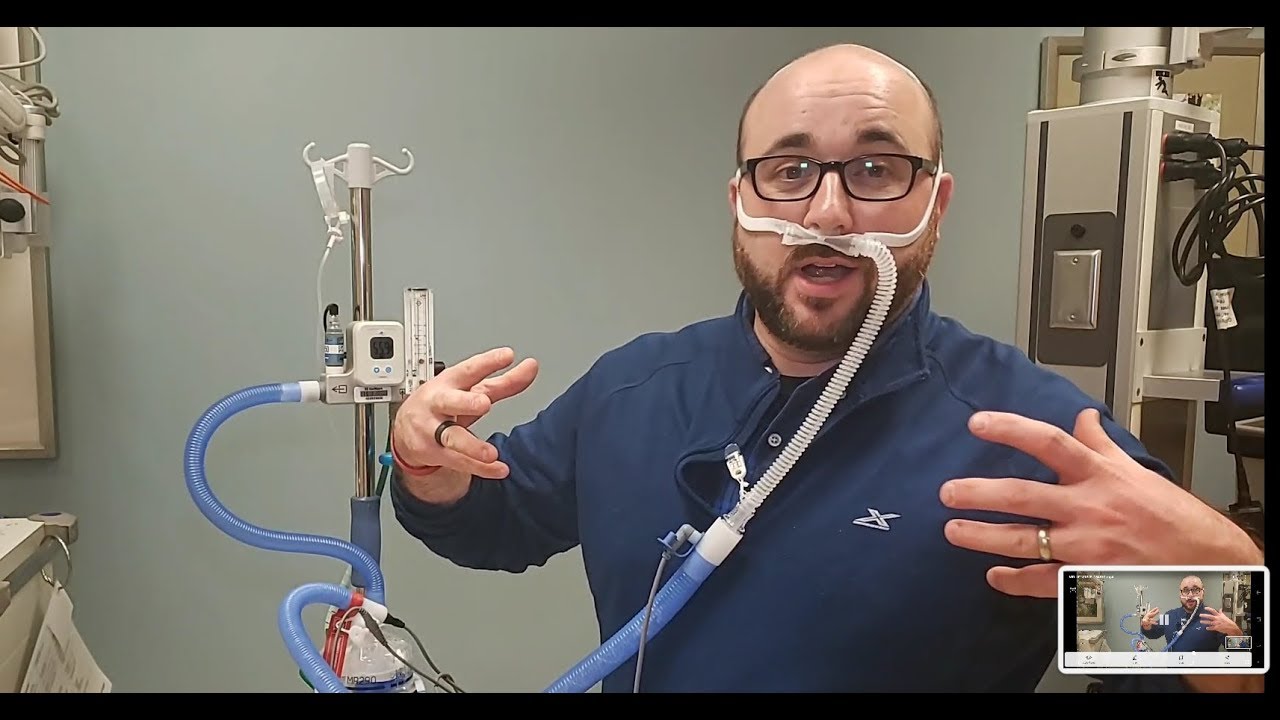
HFNO stands for High Flow Nasal Oxygen. This is something that was used frequently in patients who were desaturating quickly with symptoms of COVID-19. It has the ability, through the use of several different devices or setups, to deliver very high concentrations of supplemental oxygen to patients with advanced pulmonary diseases or conditions. In the physical therapy world, we don’t see these devices used very often unless we frequently work in ICU or with patients who have chronic disease, so I thought I would give you a run down of devices and what they look like so you can recognize HFNO when you see it and know what that implies for your interventions.
Improving the ventilation of oxygen will hopefully improve the amount of oxygen that gets diffused and perfused. This can be done by positioning, removing obstructions through airway clearance, bronchodilation to increase the space for more oxygen to get into the lungs, or by increasing the overall amount of supplemental oxygen. Given that bronchodilators can be contraindicated and/or have serious side effects and patients need something a bit faster than airway clearance techniques, supplemental oxygen tends to be a first line of treatment. This supplemental oxygen can come in different types:
Compressed gas – we typically see these green canisters everywhere, but oxygen delivered from a concentrator also fits this description.
Liquid – also called Helio, oxygen is distilled to a liquid for greater storage capacity. Hospitals typically have large storage tanks (called “dewers”) of liquid oxygen which is evaporated on site and then delivered to patient rooms on gas form. Helios can be used in the home setting, as well. The tanks look a bit different, and this is usually only used for high flow needs because compressed gas tanks run out much faster.
Compressed gas and liquid can both be run through continuous flow or “on demand” systems.
To understand high flow nasal oxygen, you need to know how much supplemental oxygen is actually being given. That depends on how many liters per minute the patient is receiving. Time to get science-y! Normal atmospheric contents break down looks like this. (See pie chart)
This matters because we have to base our supplemental oxygen calculations on “room air” which is basic inhaled air which is 21% oxygen. Every liter of supplemental oxygen added after that is roughly equal to 3% more oxygen. You can see the math is already done for you in this table.
Source: Pacer Project
You may be thinking, “I don’t know that I’ve ever seen anyone with 6L of oxygen… Doesn’t everyone just get 2 liters? That’s all I usually see…” Yes, 2 liters/min is a VERY common prescription for supplemental oxygen. But, as you can see form the table, that means the patient is only receiving 6% more oxygen than they would on room air (or with no supplemental oxygen). However, in the world of chronic disease, it is incredibly common to see 4 liters, 6 liters, and sometimes 10 liters.
These numbers can be fairly easily achieved with one or two concentrators as the standard concentrator goes up to 5 L/min (some go to 6, it depends on the brand). In the acutely chronically ill or, in the case of COVID-19, just the acutely ill, we sometimes see the need for much higher levels of supplemental oxygen. These levels cannot be achieved with the standard concentrator, so high flow equipment is brought in. Because this high flow is significantly irritating to the human tissues, it also must be heated and moisturized. So these devices must also provide this modification. Moisture can easily be added to a standard concentrator using a humidifier attachment, but this has to be ordered. You may have to request one of these for your patients to increase their oxygen compliance.
Some of the appliances and devices you’ve probably seen can be utilized to deliver high flow oxygen if necessary. A standard reservoir mask like this one (aka partial rebreather or nonrebreather depending on the construction) can deliver high concentrations of oxygen (up to 1.0 FiO2 or about equal to 25 L/min) if the flow rate is high enough. You may have seen these in emergency departments or being used by first responders.
Conserver masks can come in many different types, though, and there are some that are seen only in certain situations to deliver high flow oxygen. These masks collect oxygen in their reservoir and then feed this oxygen back to the patient at the higher collected concentration. Different types are chosen based on patient tolerance and need. These masks can be really great for patients who need to eat with their high flow oxygen because it doesn’t utilize a rebreather style mask that covers the mouth. These can also be utilized in combination with liquid oxygen (instead of with a concentrator). Liquid oxygen (sometimes called Helio) increases the amount of oxygen that can be stored in one place. Hospitals tend to have a liquid oxygen supply that is evaporated and then sent to rooms to provide oxygen to patients. These are some of the most common high flow masks I’ve worked with.
There are also some high flow devices that are a little more standard in their appearance. They look similar to a regular oxygen cannula, but they have a wider inside diameter to allow for increased flow rates.
And remember how I said that this air needs to be heated and humidified so that it’s actually tolerable? Here is the device that provides that! This is the Venturi. This bad boy can deliver anywhere from 20-60 L/min of supplemental oxygen! This oxygen at such a high flow is used to wash out dead air space like with people who have advanced COPD. This also creates a bit of PEEP to improve ventilation, like a CPAP. This is another one of those things that I wish I could have in my trunk!
This heated humid air actually helps the anatomical function of your soft tissues so they can diffuse oxygen better. Without the heat and humidity, large amounts of mucous would develop and actually block airways. This specific device actually allows clinicians to adjust the FiO2 to help prevent oxygen poisoning for those who rely on hypoxic drive. This type of device can also be helpful for your patient on BiPAP who needs to maintain saturation while eating as it utilizes a nasal delivery, so the mouth is not obstructed while the airways remain patent.
So, what does all of that mean for your therapy? Well, if a patient is on high flow oxygen and you aren’t seeing them in the hospital, odds are they have a pretty advanced stage respiratory disease. This can be COPD, cystic fibrosis, pulmonary fibrosis, or any other condition that results in chronic hypoxia. Many of these mask types are portable (with the exception of the last one pictured), but the portable oxygen supply may be short. High flow means they will run out faster. It also means that portable concentrators are probably not an option as most of them are limited at 4 L/min. High flow stationary concentrators are available that go up to 10 L/min, but your clinic would need to have one for the patient to use as they are not portable. Ultimately, this patient either needs to be connected to a wall-mounted oxygen source with a reservoir/conserver mask (this can be done in physician offices, typically), or they need to be seen at home.
If you are seeing them at home or in a sub-acute facility, this means you need to be sure of a couple things:
You are monitoring oxygen via pulse oximetry with everything, including rest
You are auscultating their lungs at every visit to assess function and/or change in presentation (pneumonia starts quickly when there is a lot of dead space or secretions)
The patient has a back up supply of oxygen somewhere that can last up to 24 hours in case of power outage (Kilo tanks or Helio)
You have educated your patient on frequency of cleaning and discarding oxygen equipment to prevent respiratory infections
You are still exercising them to an appropriate intensity (60-80% HRmax) for as long as they can tolerate
Yes, I promise, you can still exercise patients who have to utilize HFNO, even up to 85% HRmax. I’ve had patients running 16 L/min alternating squats for strength and amplitude exercises to improve their rib and spine mobility. They will get to their target heart rates pretty quickly and need their activity attenuated to maintain that level without quickly exceeding it.
(Chris Clark | Spectrum Health Beat)
Yea, that’s me doing those exercises. See that nonrebreather reservoir mask? She called it the “bag mask”. See that string hanging from my pocket? That’s my pulse oximeter. As always, she was using her 16 L/min to laugh at me.
Do you see patients who use HFNO? What are the most common diagnoses? Tell me in the comments!
Tepper, S., Wruble, E., Stewart, E. (2020). Anatomy, histophysiology, and pathophysiology of COVID-19. Pacer Project. Retrieved from https://YouTube.be/w7bafww8IWo
I’m starting to push more in to the cardiac side of things. As well as this being the original intent of this blog years ago, it is also because your focus should also be shifting. If you are treating COVID-19 patients, you need to start focusing on their heart. The patients who did a stent in the ICU are likely very deconditioned. We know that deconditioning is not just a skeletal muscle condition, it is also a cardiac muscle condition, and interventions need to target both types of muscle. So it’s time to start building up that aerobic capacity. However, if your patient is deconditioned (whether it be COVID-19 related or just plain old frailty or immobility), you need to be thinking about the effects this has on their cardiac function. Odds are they have a decreased ejection fraction (EF).
What is an Ejection Fraction?
Ejection fraction is the measure of amount of blood ejected from a heart ventricle, typically the Left ventricle is considered when we talk about EF. Questions about ejection fraction show up often on licensing exams because you really have to know the numbers to know what normal is. It’s a fine line with little wiggle room.
55% or more is considered normal 55 – 50% is considered borderline 50% or less is considered reduced
How Is Ejection Fraction Reduced?:
There are so many ways this can happen. We mentioned above about deconditioning which is probably the most common way we see this happen in so many people. But with deconditioning, there is typically an underlying cause. These can include:
Do these things sound familiar? They are all associated with heart failure. And ejections fractions are directly associated with heart failure. Like we discussed here, heart failure can come with a reduced or preserved ejection fraction. We will talk more about this in another post.
What impact does that have?
People who have decreased Left Ventricular EFs have increased health care costs! Just look at that list above: hypertension, cardiomyopathy, valve dysfunction, MI. We know those are all associated with large amounts of medical intervention including medications, rehab, and surgeries. The dollar signs amount. BUT, if you thought we just became the “frontline” against cardiopulmonary diseases due to COVID-19, you’d be wrong. Well-prescribed aerobic exercise is the key to success, recovery, and prevention for all of the items on that list. Let’s talk a little more about that.
Can Ejection Fraction be Improved?
Why, Yes. Yes it can.
Sure, there are other ways to improve ejection fraction, like:
CABG procedure. Increasing blood flow to the cardiac muscle increases its oxygenation and nutrient supply and therefore its contractile power.
Aortic Valve Replacement. If the valve is leaky, blood is flowing out when the muscle isn’t contracting, so when the muscle does contract, there isn’t as much blood left to be ejected. Replacing the valve fixes the leak.
β-Blockers (Metoprolol in particular). Stabilizing the heart rhythm improves contractility because all fibers can work together instead of having errant electrical activity interfering with contractility.
But we know these things come with other heavy medical burdens, side effects, and drug interaction risks. So the obvious best choice is going to be an intervention that decreases need for medications, prevents surgical intervention, and has little inherent risk. Enter aerobic exercise! Of course, it isn’t that simple, is it? Or everyone would be doing it on their own. People who have a reduced ejection fraction have reduced oxygenated blood flow from their heart. That means they are in the category of “having a dam built upstream”. Read this post for more on that.
Pre-surgical participation in Cardiac Rehabilitation programs decreased the cost of care for people who underwent surgical intervention. Post-surgical participation in cardiac rehab programs also decreased the cost of care for people who underwent surgical intervention. Can you imagine if we did both??? Utilizing well-prescribed aerobic exercise with appropriate vitals monitoring, functional outcome measures, and patient centered goals is going to get these patients back on track to a normal life. There, of course, are some cases where exercise is not the only answer, but it needs to be used in combination with other interventions. That’s even more reason for PTs and OTs to be involved. Our advanced knowledge of medications, comorbidities, and the effects they have on the body and exercise are what these patients really need.
Patients can’t cardiovert themselves. They can’t bypass themselves. They can’t prescribe for themselves (even though some try!). But they CAN exercise for themselves! With your professional guidance, of course! Empower them to take control.
Who does the cardiac rehabilitation at your facility or system? Tell me below in the comments!
Do you ever wonder, “did anyone else see that?” We find those red flags sometimes, don’t we? We see something odd in a physical exam and it completely changes our perspective on the patient. The key to seeing it, though, is to look for it. You may be thinking, “another thing I need to add…
Isn’t COVID-19 just a respiratory disease? If only that was true. We are good at treating respiratory infections. We have lots of drugs for viral, bacterial, parasitic, and fungal infections of the lungs. Most of them work really well! We also have several backup treatments, inhaled medications, and adjuvant therapies (like rehab!) that make primary…
Treating patients with acute and chronic clotting conditions is not new to rehabilitation professionals. We even have clinical practice guidelines around how to do so safely. However, what is new is the increased risk of newly acquired clotting conditions among post-COVID-19 patients. Those of us practicing in acute, subacute, emergency, and outpatient settings are uniquely tasked with…
Engelmeier, R. S., O’Connell, J. B., Walsh, R., Rad, N., Scanlon, P. J., & Gunnar, R. M. (1985). Improvement in symptoms and exercise tolerance by metoprolol in patients with dilated cardiomyopathy: a double-blind, randomized, placebo-controlled trial. Circulation, 72(3), 536–546. https://doi.org/10.1161/01.cir.72.3.536
Tucker, W. J., Beaudry, R. I., Liang, Y., Clark, A. M., Tomczak, C. R., Nelson, M. D., Ellingsen, O., & Haykowsky, M. J. (2019). Meta-analysis of Exercise Training on Left Ventricular Ejection Fraction in Heart Failure with Reduced Ejection Fraction: A 10-year Update. Progress in cardiovascular diseases, 62(2), 163–171. https://doi.org/10.1016/j.pcad.2018.08.006
It sounds like a fuzzy lovable Sesame Street character, but this big boy ain’t no joke. ECMO or Extracorporeal Membrane Oxygenation is basically a lung outside the body. Blood passes through it. CO2 is removed and oxygen is introduced. It sounds simple, but that is the furthest thing from the truth. This is really advanced care and should only be provided by very skilled rehab providers and their teams. I’m going to stay relatively superficial here and focus on information only. These patients are not coming home on ECMO, but there are some factors that may be relevant to your evaluation and treatment of a patient who has recently been on ECMO.
Just like we have patients we can provide external kidney function through hemodialysis and external cardiac function through cardiac bypass, we can provide support for the lungs, also. ECMO also does the pumping of the reoxygenated blood back in to the body, so it functions as a heart, too. You don’t hear much about ECMO in the rehab world, and especially not in the general public and daily conversation. But lately, thanks to COVID-19, that is changing. So, here are the basics of what you need to know about ECMO and what to consider if your patient is coming to you after a stent with the ECMO monster.
My first experience with ECMO was during my time as a heart and lung transplant educator. One of my long time patients had been pre-habbing toward bilateral lung and vasculature transplant due to pulmonary hypertension and COPD. I visited her in the hospital after her transplant was completed and she was on ECMO. The tower next to the bed was breathing for her instead of her own brand spanking new lungs. Large plastic hoses were running out from under the sheets into the machine and then from the machine back in to her. It was a startling sight. Thankfully, the next time I saw her was in her home, and she was sitting up and singing just like she had been before the transplant.
Basically, ECMO is a last-ditch effort, a last resort. If mechanical ventilation isn’t working, even at the highest settings considered safe, ECMO may be brought in. This takes a huge effort, a large team, and round-the-clock monitoring of the machine and the patient. Typically, only very highly skilled teams and facilities are able to provide ECMO. ECMO is by no means a highly successful intervention. A recent study of patients with COVID-19 demonstrated less than 50% of people who were placed on ECMO survived (21 of 58). And let’s not forget that “survival” doesn’t mean they popped up and raced home to their family. ECMO also extends the road to recovery for most patients. However, that could be seen as a percentage of people who survived that would have otherwise died on the ventilator, so we can definitely see the benefit.
So why isn’t every patient failing mechanical ventilation, whether it be due to new onset GBS or succumbing to viral overload, given ECMO? We don’t have the resources. We don’t have the people. Like I said above, utilizing this device takes a team. This team includes twenty-four hour monitoring, usually in the room, by a respiratory therapist or registered nurse who specializes in pulmonary care. A surgeon and surgical team are required to implant the hoses in to the patient’s vasculature (no small feat). Several physicians also must come together to make the decisions on when is the right time, who are the right patients, and who has the best chance of survival. These are just the extras. This is all in addition to the already stretched team of nurses, nursing assistants, hospitalists, social workers, and rehab therapists that are working with the patient. And, prior to COVID-19, we didn’t have hundreds of patients at a single hospital going in to ARDS at one time, so we don’t have that many ECMO machines sitting around.
You can see more about the guidelines for use of ECMO here:
The ECMO machine I’m more used to seeing. (credit)
Now, down to the meat and potatoes. What does rehab look like with ECMO? It depends (of course). Many times, patients are heavily sedated while on ECMO. But, sometimes, they aren’t. Sometimes they are able to be functional and awake and they need you so much at that point in time. Placing and managing ECMO takes a team, but so does rehab during ECMO. I want you to know what it looks like to ambulate a patient on ECMO, so please watch the video at this link.
Things you need to consider when evaluating a patient who has recently had ECMO:
Wounds. Several vascular access sites will still be healing. You may find them in the neck, chest, or upper thighs. Access can be placed in the femoral veins or jugular veins depending on the needs of the patient and the machinery available. These wounds place the patient at an increased risk of sepsis so they need to be carefully monitored for healing and/or signs of infection, dehiscence, or delayed healing. If they were on ECMO, odds are they had several other support devices in place (you saw those pictures and videos), so there will be several other vascular access sites not for ECMO and the same considerations apply. I’ve seen IV sites become infected and cellulitis spread through an arm because of it. Venipuncture sites matter just as much as surgical wounds. More research coming out is showing soft tissue infections as one of the main factors for returning to the hospital after discharge.
ProfoundWeakness. I’m not talking your average deconditioning. These patients were likely “under water” and/or sedated for several weeks, being completely dependent for all movement. Specifically for patients with COVID-19, the small muscles (intrinsics, muscles of the lower arm and legs) and core musculature seem to be greater challenged than the large musculature. Their diaphragms have done NOTHING for a long time and their cardiac function has been so chemically modified that the muscles don’t even know what to do anymore. Don’t forget about your tools like IMT and PEP to help with this! Supplemental oxygen can typically be run through these devices if needed.These patients need a greater level of reconditioning, a longer timeframe of overall recovery, and they are starting from an even further place than their non-ECMO cohorts with COVID-19. They need coordination training for the muscles of breathing and the cardiac system and they need to take it low and slow. You can find more information about that here.
Delirium. Just mechanical ventilation can cause delirium. Just ARDS can cause delirium. A hypoxic state can cause delirium. So imagine if you have all of those things and then you get put WAY WAY under so that a machine can oxygenate your body. The delirium is going to be there and it’s going to hang on for a while. There are many measurement tools that can be appropriate for establishing level of delirium, but the important thing is that you quantify a baseline so you can show improvement in delirium over time. Keep in mind that there may be little to know carryover or ability to generalize any skills instructed due to the “fog” still present. It has been postulated that these patients present very much like patients after traumatic brain injury and that the Richmond Agitation and Sedation Scale (RASS) used frequently in ICU settings may line up well with the Ranchos Los Amigos Scale/Levels of Cognitive Functional Scale (RLAS/LCFS) used in patients with TBI. It has been noted by several ICU practitioners that these patients really do present as if they have experienced a traumatic brain injury. Based on this, you have to modify your lens through which you view the patient, their participation, your activities, and your therapeutic goals. Those Neuro skills are really going to come in handy!
What was your reaction when you first saw an ECMO machine attached to a patient? Tell me about it in the comments!
If there is any treatment that I feel like gets used in a cookie-cutter fashion, it’s pursed-lip breathing. As much as I hate seeing this technique used for every single patient that has shortness of breath, it does have clinical usefulness. So let’s talk about how to implement pursed-lip breathing properly based on patient presentation…
We’ve all seen that dreaded picture in our textbooks… All the human figures laying in so many different positions with pillows and tables tilted all over… and I very clearly remember thinking, “How on earth am I supposed to remember all of those?” Well, good news. You really don’t have to. It’s great if you…
Lin K, Wroten M. Ranchos Los Amigos. [Updated 2019 May 29]. In: SatPearls. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448151/
Seethala, R. & Keller, S. P. (2020). ECMO resource planning in the setting of pandemic respiratory illness. ANNALSATS Articles in Press. American Thoracic Society. doi: 10.1513/AnnalsATS.202003-233PS. Retrieved from https://www.atsjournals.org/doi/pdf/10.1513/AnnalsATS.202003-233PS
The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients.Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O’Neal PV, Keane KA, Tesoro EP, Elswick RKAm J Respir Crit Care Med. 2002 Nov 15; 166(10):1338-44. https://pubmed.ncbi.nlm.nih.gov/12421743/
I know you are hearing this phrase a lot lately. We are hearing all the time that, as things open up around our country and around that world, we may experience a second wave resurgence of new COVID-19 cases. But I’m not referring to a second wave of new COVID-19 patients. There is new research coming out regarding patients who had previously experienced COVID-19 being readmitted to the hospital for a second wave of symptoms. These people have gone home. They have been discharged. They have recovered to a functional point. And yet, here they come, back in to the Emergency Department showing symptoms of COVID all over again. Why? What is going on here?
My first thought when I read this article was, “Here we go as a healthcare system, sending people home too soon again, just like we have been pushed so hard to do.” I was making some assumptions based on what I already knew, but what was really going on? Turns out I wasn’t wrong. Those with shorter median length of ICU stay (less than 5 days) were more likely to return for care, however, they were also more likely to not require readmission. They just needed some extra support like NIV/NIPPV, medication, breathing treatments, etc, and then were discharged from emergency back to home. In addition to length of stay, there are some significant factors that can result in patients being at a higher risk of readmission after COVID-19 discharge. Let’s take a look at what those are so you can better inform your practice and keep a closer eye on these folks.
First off, WHY are these patients returning to the hospital after discharge? The most common reason is a resurgence in respiratory distress. Other reasons included chest pain, falls, soft tissue infections (We will talk more about this in an upcoming post), and altered mental status. Patients tended to return to the hospital within 4-5 days of discharge so this seems to be the high-risk time frame. There were also a few specific conditions and comorbidities that resulted in a higher risk of returning to the hospital after COVID-19.
Not surprisingly, patients who have a comorbidity of COPD had a higher risk of returning to the hospital after COVID-19 discharge (6.8% of returning patients). These patients already have a compromised respiratory system so incurring further damage from viral overload isn’t going to do them any favors. These patents are more likely to require advanced ventilatory support, are more likely to experience severe disease, and are more likely to have a negative overall outcome, so returning to the hospital is not unexpected.
What was a bit surprising is that patients with hypertension were even more likely to return to the hospital than patients with COPD (36% of returning patients)! The mechanism for this continues to remain unknown. However, if you consider the effects of COVID-19 on the circulatory system that we discussed in my post on DVTs, we can infer that the heart and vasculature are struggling for a number of reasons. Down this line of thinking, another factor that placed patients at a higher risk for readmission was whether or not they received anticoagulation therapy… Hmmmmm…
Lower BMI at hospital discharge was also associated with higher risk of return to the hospital. It was assumed in the article that the effects of frailty impacted the readmission rates. But, in addition to frailty, which is a defined system of events and presentations, I think we need to consider the effect significant muscle mass loss has on BMI. Because these patients are immobilized for a long period of time, they are more likely to lose significant amounts of muscle mass which then lowers their overall BMI (which is body mass in kg per cm of height). So, if you have a patient who has a large proportion of muscle mass at admission, and a low proportion of muscle mass on discharge, regardless of comorbidities or age, they may be at a higher risk of readmission.
Thankfully less than 4% of people who were discharged from the hospital after COVID-19 returned to the hospital. But for those 4%, more than half required readmission to the ICU, so if they do end up going back, they are probably in dire need of help.
For all of you out there treating patients who have returned home or to a sub-acute facility and are in that 5-ish day window after discharge, you need to be keeping an extra special eye on them if they have COPD, hypertension, low BMI, a shorter ICU stay, or did not receive anticoagulation therapy. Did I just name every home care patient? Maybe…
Have any of your patients gone back to the ED after being discharged for COVID-19? Tell me about it in the comments!
This article can be read for free on MedBridge! Click the link below! Could the cardiotoxic effects of monocloncal antibody treatment be contributing to the ongoing effects experienced by those with long COVID? Let me know what you think in the comments!
I took a trip to Denver recently and, right around the same time, was consulted regarding the use of a pulse oximeter at high altitudes. It all got me thinking: how different could it really be to practice at 9,000ft? So, I did some work on this and I have to tell you, finding this…
I hope, at this point, you’ve all heard of the FAST acronym for identifying signs of a cerebrovascular accident (aka stroke). My in-laws even have a magnet on their fridge with a great comic strip describing the FAST acronym. I have run in to a couple different versions of it in the last few years,…
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!
References:
Somani, S., Richter, F., Fuster, V., De Freitas, J., Naik, N., Sigel, K., Boettinger, E. P., Levin, M. A., Fayad, Z., Just, A. C., Charney, A., Zhao, S., Glicksberg, B. S., Lala, A., Nadkarni, G. (2020). Characterization of Patients Who Return to Hospital Following Discharge from Hospitalization For COVID-19. MedRxiv [Pre-Print Release]. Retrieved from https://www.medrxiv.org/content/10.1101/2020.05.17.20104604v1.full.pdf+html
Thanks for tuning in to part 2 of this two-part feature of VTE. The first segment, which focuses on DVTs, can be found here!
So now we are going to focus on the more critical version of a VTE. Yes, DVTs are critical. They are important to assess and treat quickly. But they are less acutely life threatening than a pulmonary embolism. Let’s take a closer look at PEs and how they are relevant to rehab clinicians.
A pulmonary embolism is something (usually a blood clot) that moves through the vasculature and eventually impedes a vessel that supplies a portion of the lung. This sudden blockage is typically a clot, but can potentially be several different things such as fat, bone, soft tissue, air, etc. You may be thinking, “How would any of those things get in to an artery and cause a blockage in the lungs?” Well, through external means. People who undergo surgeries are at an increased risk for PE because the act of cutting through tissue can introduce those elements in to the arterial system. Crush injuries can also introduce tissues in to the vasculature that doesn’t belong there. If these insults are relatively small enough to pass through our peripheral vasculature, they can make it back to the heart, and are then pumped into the pulmonary arterial supply. The emboli are actually pretty large because they are typically formed in the deep leg veins (they start as DVTs) which then dislodge and travel back to the heart through our relatively larger veins. However, vessels in the lungs get very small very quickly (they have to be capillary sized to perform oxygen and CO2 diffusion at the site of alveoli), so blockages are likely to happen here.
Just like with DVTs, PEs have a particular set of symptoms that can be quantified on a couple different scales. Like we talked about in the first post, the Wells’ Criteria has a scale for PE risk assessment. It works pretty much the same as the DVT risk assessment and the criteria are similar. As you can see here, I’ve set the tool for an assessment of a patient with COVID-19 with a typical presentation. However, this score could also be given to a patient after a joint replacement as the assessment would look very similar. The bonus to using the Wells’ Criteria is that it factors in the clinical gestalt. We mentioned this briefly in the last post. Your gestalt has been researched thoroughly and it has actually been shown that clinical gestalt (the feeling that something is amiss) is actually the single most important clinical tool in determining the need for further workup. If all your tools are telling you everything is fine, but you feel something is wrong, something is probably wrong, and there is research to back that up.
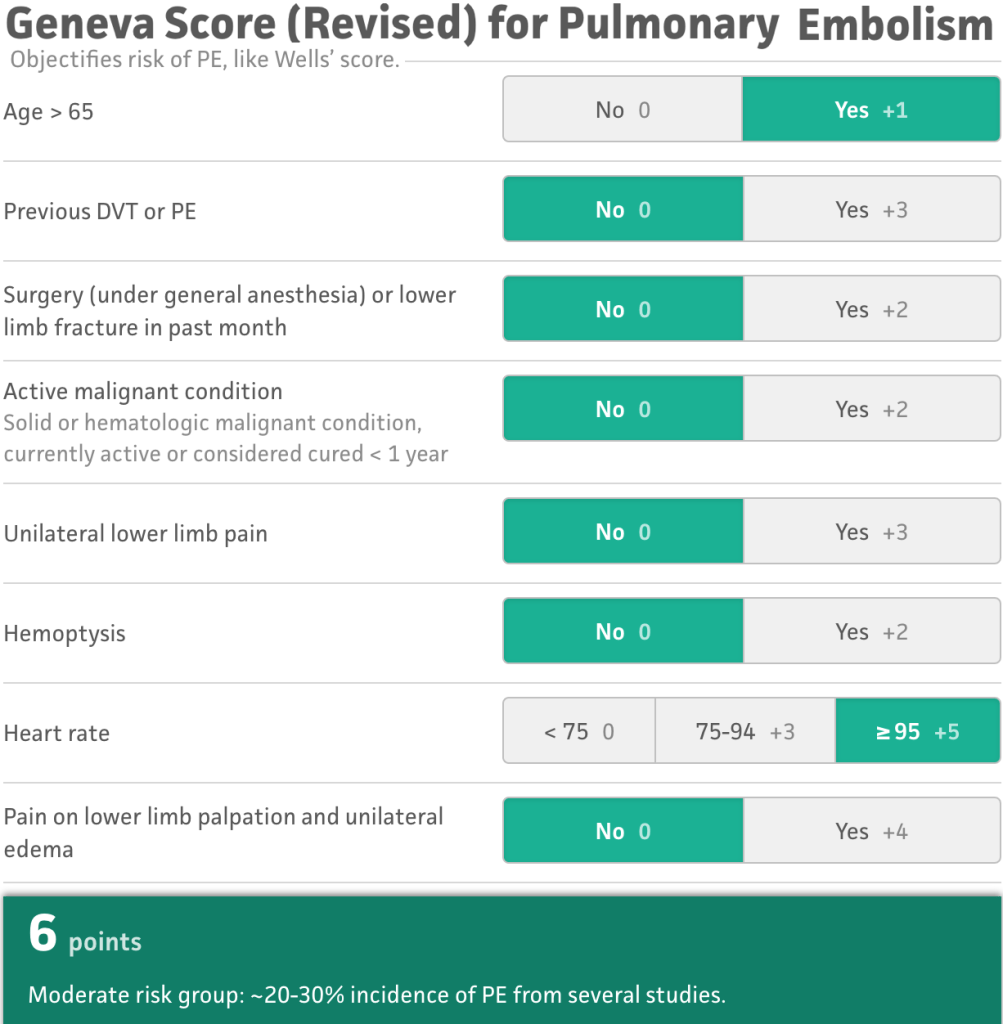
Another tool becoming more commonly used is the Revised Geneva Tool (rGeneva). Meta-Analysis outcomes have shown that the rGeneva is actually just as accurate in predicting risk of PE being present as the Wells’ criteria. The difference between the tools is that the rGeneva stratifies risk across three categories (low, medium, and high). The original version of the rGeneva utilized outcomes of ABGs and other assessments that take precious time to order, measure, and interpret, so the tool was revised to be done with only a physical patient assessment. This tool does not weigh clinician gestalt, so it is felt to have less clinical strength than the Wells’ Criteria, however, still very valid and useful.
How to inform your gestalt
There are some clinical factors that should be informing your gestalt when it comes to pulmonary emboli, some physical assessment pieces that should take you down the road of either ruling this out or calling 911. In a patient who has been immobilized or with recent surgery, the most obvious signs would include:
Shortness of breath at rest or with minimal exertion
(believe it or not, shortness of breath is NOT ALWAYS PRESENT in patients with pulmonary emboli!)
Tachycardia and tachypnea
Significant decline in functional status
Confusion
Chest pain with breathing (pleuritic pain) (65% of patients)
If these factors are coming up in your physical exam, patient interview, or functional assessment, you should be very concerned and doing some deeper digging, as well as probably contacting a physician right away to report findings.
So, since I seem to have a patient or two with just about everything, yes, I’ve had several patients where I have identified a new PE. Two were post-surgical (cervical spine fusion and knee replacement), one was severely ill with end-stage COPD, and one was young but immobilized long term due to primary progressive MS. Two of these four died upon reaching the hospital. The patient with the cervical spine fusion had three PEs on his imaging but made it! The one with COPD didn’t return home. All of them were confused, some severely confused, three had a sense of impending doom, all four had abnormal lung auscultation, three had leg swelling. No one had a cough or difficulty breathing.
What happens next?
So we think our patient may have a PE. We’ve called the doctor or sent them to emergency. What happens to them now? They will get some blood work done (a D-dimer and ABGs) and some imaging studies performed. Likely, a CT angiography will be performed. I don’t know if you guys have ever seen an angiogram for a PE, but the images produced are just completely amazing and the clots tend to be pretty obvious. In the image below, image a is a slice of the pulmonary vasculature. The vessel heading off to the right (superior vena cava) is occluded with a large embolism (the shaded tubular shaped area within the white space). And image b is just incredible, but all those tiny dark spots within the white space (the vessels) are subsequent emboli.
This is obviously a large embolus. Emboli that are very large like this one present in the large vasculature can cause major damage as they block such a large vessel which means every other lower-order vessel is now also blocked. These type of emboli tend to emanate from the deep leg veins and are more common in patients who have heart rhythm issues (another reason beta-blockers are so important!). You can see in the assessment tools that there are other factors that increase the risk for developing PEs:
Cancer
Cardiovascular disease
Disorders that affect clotting
Pregnancy
That last one is interesting. While living in West Michigan, I regularly encountered patients who had a condition called Factor V. People of European Caucasian decent have an increased risk of carrying a genetic mutation that results in Factor V Leiden, a clotting factor malfunction. This results in an increase in the risk of clotting including DVTs and PEs. There are thousands of clotting disorders out there that increase the risk of clotting.
Preventing PEs
Sometimes there just isn’t much you can do. PEs are one of those things that can pop up over night and have no symptoms until someone is so far gone that you aren’t sure if they are coming back. I’ve had a patient with no symptoms one day, and the next day I had to send him straight to emergency. There are some things we can do to lower the risk, and this list is going to look pretty similar to the list for DVT prevention:
Promote mobility programs
Promote anticoagulation adherence
Promote rhythm drug adherence
Graduated compression stockings
Frequent position chages
Educate patient on signs and symptoms
Alternating pressure/compression devices
Smoking cessation
Weight loss
Does COVID-19 increase the risk for PEs?
As part of DIC (disseminated intravascular coagulopathy), the quick answer is yes. For more on DIC, see the first post in the VTE series. A new study found that 23% of patients in the ICU with COVID-19 had PEs. And I mean several PEs, not just one or two. The presence of PEs was difficult to determine due to the patient’s COVID-19 symptoms so angiography was typically performed much later than usual. The presence of PEs was determined to increase the need for and length of mechanical ventilation.
I wanted to show you some imaging for comparison. You saw the image above of the PEs in otherwise normal lungs. Below you will see what lungs look like when they not only have several PEs, but all the sequelae of COVID-19 including bronchiectasis, ground glass opacities, consolidation, and actual architectural breakdown. This particular set of lungs was thought to have a fluid volume of between 25-50%. You don’t even have to know the specifics of what all of that means to look and this set of images and realize this person is in rough shape.
Other studies have shown that between 20-30% of all patients with COVID-19 may have PEs whether they are in the ICU or not. In Detroit, doctors diagnosed 51% of the COVID-19-related PEs in the emergency department and 72% of them did not require ICU admission. However, what this can be interpreted as meaning is that even if your patient isn’t critically ill with COVID-19, their risk of having a PE is still very high.
So if you are seeing patients in the outpatient, home, or sub-acute settings, not only does their risk of having a PE or DVT increase simply because they had COVID-19, but the risk stays high and hospitalization for COVID-19 is not a factor is their PE risk. Even in patients who were on prophylactic treatment for clotting, almost a quarter of them still developed PEs. Rehab clinicians need to be watching out for the signs and symptoms of PE and DVT for any and all patients who are being treated after COVID-19 diagnosis or suspected COVID-19.
Have you ever spotted a PE? Tell me about it in the comments!
How many times have you had your temperature taken lately? I think I’ve had my temperature taken thousands of times in the last few months. We are seeing the increased use of forehead scanning thermometers and temporal scanners, all the non-contact forms of temperature assessment, to screen folks for COVID-19 symptoms upon entry to any…
I started this venture back in March in response to COVID-19. I saw many Physical Therapists and other rehab professionals shutting their doors because it wasn’t safe to keep them open. I saw an opportunity to improve our profession by addressing a deficit in practice: the lack of cardiopulmonary skill implementation. It wasn’t even that…
What is a huff? Huffing is one of the more difficulty techniques to learn for airway clearance. I find that most of my patients have trouble mustering the strength to perform a good solid huff. It’s not just that it is unfamiliar, but also that it takes diaphragm strength that they just don’t have. But…
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!
References:
Ceriani, E., Combescure, C., Le Gal, G., Nendaz, M., Perneger, T., Bounameaux, H., Perrier, A., & Righini, M. (2010). Clinical prediction rules for pulmonary embolism: a systematic review and meta-analysis. Journal of thrombosis and haemostasis : JTH, 8(5), 957–970. https://doi.org/10.1111/j.1538-7836.2010.03801.x
Grillet, F., Behr, J., Calame, P., Aubry, S., Delabrousse, E. (2020). Acute pulmonary embolism associated with COVID-19 pneumonia detected by pulmonary CT angiography. Radiography. ePub online ahead of print. Retrieved from https://doi.org/10.1148/radiol.2020201544
Le Gal, G. (2020). Geneva score (revised) for pulmonary embolism. Retrieved from mdcalc.com/geneva-score-revised-pulmonary-embolism#creator-insights
Penaloza, A., Verschuren, F., Meyer, G., Quentin-Georget, S., Soulie, C., Thys, F., & Roy, P. M. (2013). Comparison of the unstructured clinician gestalt, the wells score, and the revised Geneva score to estimate pretest probability for suspected pulmonary embolism. Annals of emergency medicine, 62(2), 117–124.e2. https://doi.org/10.1016/j.annemergmed.2012.11.002
Poyiadji, N., Cormier, P., Patel, P.Y., Hadied, M.O., Bhargava, P., Khanna, K., Nadig, J., Keimig, T., Spizarny, D., Reeser, N., Klochko, C., Peterson, E.L., Song, T. (2020). Acute pulmonary embolism and COVID-19 (a research letter). Radiology. Retrieved from https://pubs.rsna.org/doi/pdf/10.1148/radiol.2020201955
Stein, P. D., Beemath, A., Matta, F., Weg, J. G., Yusen, R. D., Hales, C. A., Hull, R. D., Leeper, K. V., Jr, Sostman, H. D., Tapson, V. F., Buckley, J. D., Gottschalk, A., Goodman, L. R., Wakefied, T. W., & Woodard, P. K. (2007). Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. The American journal of medicine, 120(10), 871–879. https://doi.org/10.1016/j.amjmed.2007.03.024
We used to think of this as only being associated with the flu. But we know now that GBS can be associated with any insult to the immune system, known or unknown (unknown in up to 40% of cases!). Now that we know COVID-19 can present, especially early on, with neurological symptoms, we need to go deeper in to this topic. So far, I have not only treated several patients in the inpatient acute and home sub-acute settings with GBS, but I’ve also identified a new onset of GBS in a patient I was seeing for neck pain after a cold. The longer I practice, the more GBS I run in to and it makes it feel like it is more common than it really is. But the actual incidence is 1-2 in 100,000. That’s pretty typical, to have your bias influenced by your experience. I always feel like everyone I see over the age of 70 needs to have a walker or cane to be safe, because those are the people I typically see for therapy, but we all know that isn’t the case in real life.
Like I started saying, GBS is one form of acute inflammatory demyelinating polyneuropathy (AIDP) which can be brought on by an insult to the immune system. For a refresher, the myelin sheath on a nerve is what promotes saltatory conduction, the process by which we can transmit neurological impulses so quickly throughout our nervous system. GBS typically takes between 3 days and 6 weeks to present after a respiratory or gastrointestinal system infection (that’s a large time-span, I know). I’ve also seen patients with GBS after a cold, the flu, or a tick bite. Guillain-Barre Syndrome can also be triggered as a reaction to a new drug. Make no mistake, even though some cases can be minor, new onset is a medical emergency.
Some diagnoses require you as a clinician to be more vigilant in your screening and ongoing monitoring for GBS symptoms, as they are more regularly associated with onset of GBS. These include:
There is no known cure, although treatment with intravenous immunoglobulin (IVIg) and plasma exchange can decrease the length of symptoms. Some patients (25-30%) will require mechanical ventilation as the ascending demyelination progresses to their phrenic nerve and higher, resulting in diaphragm paresis/paralysis and ultimately ARDS. Cranial nerves can also become affected by GBS.
So what do you need to be on the lookout for?
Most patients develop sensory symptoms first. This is an ascending demyelination, so symptoms tend to start most peripherally. Sensory changes in the fingers or toes are most common. As sensory changes progress cranially, motor deficits begin to present. The real trouble that most people run in to is when the demyelination reaches their phrenic nerve, as this is the point they lose diaphragm control and are no longer able to breathe independently. As you saw above 25-30% of patients with GBS reach this point and require mechanical ventilation. The demyelination doesn’t necessarily stop there and not everyone responds to IVIg. And then we wait. We just wait until the demyelination stops.
Now, this is the typical presentation, but that doesn’t mean you can dismiss other odd symptoms. Like I mentioned above, I was seeing a patient in the home for neck pain and difficulty walking. I was thinking some major spinal insult at the time or a stroke, but her symptoms changed at every visit. Some days she could walk just fine with a cane, other days she could hardly stand. She had no sensory deficits at all and her neurological screening was unremarkable. She only had mild proximal lower extremity weakness. When I started seeing her, repeated cervical retraction actually improved all of her disabilities, including her leg strength, so I chased that rabbit. We went from non-ambulatory to walking without deviation in one visit.
It wasn’t until the fourth visit that she started reporting sensory changes in her thighs. I thought this seemed odd, but her light touch was diminished. I scheduled some extra visits and decided to see her the next day to assess changes. Huge bells were ringing but she continued to respond to mechanical interventions and I had nothing concrete, just gestalt. The next day, she had no light touch in her thighs (no dermatomal pattern) and she reported paresthesias in her groin, along with new onset of urinary incontinence overnight. This was the moment. This was when I realized not just how bad this was but WHAT this was. The red flag had finally waved. The kicker was that she STILL responded to mechanical interventions!!! Repeated cervical retraction STILL improved her function!!!
But no matter, I had realized what this was and I knew I had to get her to a hospital ASAP to slow the progression and provide her with ventilatory support if needed. I called the PCP and reported an ascending paresthesia with intermittent paresis and paralysis of atypical presentation three weeks after a cold and her reaction was immediate. Between the PCP, the nurse, and I, we got the patient direct-admitted to the hospital within the hour. The CSF specimen obtained from a lumbar puncture showed a result consistent with GBS. I picked her back up for home therapy four weeks later. She hadn’t progressed to a vent, thankfully, but she was in the hospital and rehab that whole time.
Why are we more concerned with COVID-19?
Patients are now experiencing neurological effects of COVID-19 before, during, and after hospitalization for treatment. They may have even been experiencing them before we realized COVID-19 was the cause. From encephalopathies to ischemic strokes, the neurological complications are becoming more clear and the rehab community is jumping in to action. If you were practicing prior to COVID-19 and you didn’t do much treatment for cardiopulmonary conditions, your neurological skills may now need to be front and center.
The numbers are climbing. There are now several reported cases in Italy and the US where patients with COVID-19 develop GBS. Two new cases have even come forth in children (as of July, 2020). Some considerations are also being given to the presence of GBS as part of the initial respiratory failure. As COVID-19 can be present for up to 14 days without symptoms, that gives GBS more than enough time to develop (the 3 day to 6 week window after infection). According to the physicians who identified these cases in Italy, GBS onset was between 5 and 10 days after the first COVID-19 symptom presented (significantly before PICS should be considered).
Some physicians have asserted that GBS may be copresent during the rebounding phase of COVID-19 when patients are still on mechanical ventilation but progressing back toward functional respirations. Some patients present with a regression of respiratory function during this time that may be due to GBS, but the patient is sedated and heavily medicated and ICUAW may already be a factor so paresis is not a reliable indicator. If chest radiographs are clearing but respiratory function is declining, GBS should be a strong consideration. This also means that it may be seriously under-reported in patients with COVID-19, as it may appear as if the patient is regressing or failing the ventilator.
Where we may run in to some complications with treating GBS in patients with COVID-19 is if they have pre-existing contraindications for the effective interventions. For example, if someone has an active infection persisting (like the SARS-CoV2-19 virus for example) they cannot utilize plasma exchange. The same is true if they have issues with hemorrhage or clotting deficiency which we know can be an issue with COVID-19. Patients cannot utilize IVIg therapy if they have renal failure. We know that around 30% of patients with COVID-19 experience renal failure requiring dialysis support. So even if we can distinguish between side effects of COVID-19 and new onset GBS, we may not be able to do anything about it. This would significantly extend the length of recovery time.
Speaking of recovery…
That’s really where we come in, isn’t it! Guillain-Barre comes with a host of neuromusculoskeletal impairments and functional limitations that require skilled rehabilitation. You can imagine that when neurological signals are slowed down significantly, our internal communication system literally bogs down, all the end organs just don’t function properly. You can expect your interventions to target (at minimum):
Sensory deficits, specifically proprioception
Balance impairments in seated, standing, and dynamically
Overall lowered functional status
Impaired trunk control
Let’s start off by performing a neurological baseline assessment here. You have to figure out where you are starting from. Talk to your patient about their goals, what they need to get home, what they want to return to doing, and build on that. The Berg Balance Scale, although not my choice balance assessment, is the most studied in recent GBS research, and correlates with other testing. But perform what tests you think are most meaningful to your patient, reflect their true functional deficits, and include items that they are required to do in their normal life. If they are still at a seated level of function in acute rehab, the FIST is a great tool to start with. But you can also do a full-system assessment with the BESTest in any setting. Also keep in mind that you may need to do some testing for the cardiovascular system, like an aerobic capacity test, if your patient also has COVID-19 (or just had influenza or pneumonia or any other respiratory insult).
When it comes to strengthening, you have to consider the neurological anatomy that has been damaged. We know it takes nerves forever to regrow after damage, and that’s after Wallerian degeneration has completed. In GBS, the full nerve structure has not been damaged, just demyelinated. But this still will take a while to heal, especially in the presence of a hypoxemic comorbidity, as reduced overall tissue oxygenation also affects the neurological system. So strengthening should be focused on functional tasks and monitored closely as the patient can be expected to fatigue quickly due to poor recruitment. We usually hear that you should avoid eccentric exercises in this population for this reason. High-Intensity exercise was shown to improve outcomes across all systems relative to lower intensity exercise in patients with GBS. However, there is very little well-controlled research for interventions for these patients.
In the long term, rehab is indicated and expected to take place over an extended period of time with GBS alone. Very recent research has shown that physical therapy interventions are most successful if provided for greater than six months with patients who have experienced GBS. When you factor in a respiratory virus and subsequent sequelae (like the effects of mechanical ventilation or PICS), we can expect a long return to function time frame. Set your patient up for success by setting achievable and reasonable goals. Break your time frames down and try to achieve goals every week and make sure your patient KNOWS they are achieving goals and making progress. The road is long, but the news is good! 85% of people with Guillain-Barre Syndrome make a full recovery.
What is your favorite strengthening exercise to use with patients who have had Guillain-Barre Syndrome? Tell me about it in the comments!
Follow @DoctorBthePT on Twitter for regular updates!
References
Arsenault, N. S., Vincent, P. O., Yu, B. H. S., Bastien, R., Sweeney, A., Zhu, S. (2016) Influence of exercise on patients with Guillain-Barré Syndrome: a systematic review. Physiotherapy Canada. 68(4):367-376. https://www.utpjournals.press/doi/abs/10.3138/ptc.2015-58
Head, V. A., & Wakerley, B. R. (2016). Guillain-Barré syndrome in general practice: clinical features suggestive of early diagnosis. The British journal of general practice : the journal of the Royal College of General Practitioners, 66(645), 218–219. https://doi.org/10.3399/bjgp16X684733
Huzmeli, E.D., Korkmaz, N.C., Duman, T., Gokcek O. (2018). Effects of sensory deficits on balance, functional status and trunk control in patients diagnosed with guillain-barre syndrome. Neurosciences. 23(4):301-307. doi: 10.17712/nsj.2018.4.20180098.
Prada, V., Massa, F., Salerno, A., Fregosi, D., Beronio, A., Serrati, C., Mannironi, A., Mancardi, G., Schenone, A., Benedetti, L. (2020). Importance of intensive and prolonged rehabilitative treatment on the Guillain-Barrè syndrome long-term outcome: a retrospective study. Neurol Sci. 41(2):321-327. doi: 10.1007/s10072-019-04077-x. Epub 2019 Oct 4.
Sharshar, T. (n.d.) Guillain-Barre Syndrome. [Presentation]. University of Versailles – Saint Quentin en Yvelines, Raymond Poincare Teaching Hospital. [French Neuro-Anesthesia and Resuscitation Association]. Garches, France. Retrieved fromhttp://www.anarlf.eu/medias/slideshows/fichiers/GBS-DIU-Lyon-2015.pdf
Toscano, G., Palmerini, F., Ravaglia, S., Ruiz, L., Invernizzi, P., Cuzzoni, M.G., Franciotta, D., Baldanti, F., Daturi, R., Postorino, P., Cavallini, A., Micieli, G. (2020). Guillain–Barré Syndrome associated with SARS-CoV-2. NEJM. Retrieved from https://www.nejm.org/doi/full/10.1056/NEJMc2009191
Zhao, H., Shen, D., Zhou, H., Liu, J., Chen, S. (2020) Guillain-Barré syndrome associated with SARS-CoV-2 infection: causality or coincidence? Neurology Lancet. Retrieved from https://doi.org/10.1016/S1474-4422(20)30109-5
No, I’m not sick or symptomatic or high risk or any of those things. As some of you know, after six years working home health, I recently transitioned to a long term care and skilled nursing setting. Governmental changes made testing mandatory for all providers, staff, and volunteers in these settings. I’m not going to comment on the personal factors and feelings toward mandatory testing, and for good reason: It’s mandatory. It doesn’t matter what my feelings are. If I want to work, I will be tested. The same goes for TB, and I get tested for that yearly. So today, I was tested for COVID-19. I’m sure many of you are going to be tested soon, or maybe you already have been! But here are some things I can explain and clear up for you based on my experience.
There is some paperwork. Ha! Is that a surprise??? Like all medicine and healthcare, there is plenty of paperwork to go around. I signed three different consent forms prior to being tested. Nothing was out of the ordinary, just standard language about HIPAA stuff, who is performing the testing, how the samples will be handled, when and how you will be notified of results… And then, you know, the standard informed consent stuff we give to all our own patients such as symptom descriptions, when to contact your doctor, possible side effects of testing…
It doesn’t hurt. Speaking of side effects… I know, lots of people are out there saying they feel like they are having their brains swabbed. But, I can tell you from experience now that it is not painful. It feels more like you have a righteous sneeze coming on. I mean, they are tickling the inside of your nasal passages with a tiny plastic brush so that’s really not surprising. Maybe, if you are super sensitive, you may get mild discomfort for 10 seconds, but I can’t imagine anything other than that. (Exceptions for those who are tested often due to frequent exposures. I feel like that could get really annoying.)
They swab both sides. That tiny little plastic brush will go up both sides of your nose so your nasal passages will be thoroughly and equally tickled. They brush really is tiny. Nothing crazy. It looks like the same one my pediatrician uses to test my kids for the flu.
Everything is super clean. As you can see in the pictures, everything is individually packaged in sanitized packaging, bleach wipes are there, hand sanitizer is used… These testers came fully equipped with gowns, shoe covers, gloves, body suits, shields, and N95s. They probably had more PPE between the 5 of them than some clinics I’ve been to. They were testing many of us today, so they definitely came prepared.
It is fast. I was in and out in less than 10 minutes and that included a quick stop to chat with my boss and a coworker, as well as time to fill out the paperwork and get my screening temperature taken. The actual test was less than 30 seconds. This really couldn’t be easier. You just have to stand there.
Results take three days. So now that testing is over, the suspense begins. I get to just sit back and wait. I’m not worried, like I said, I’m not symptomatic. I’m actually glad to be tested because the last thing I’d want is to be an asymptomatic carrier and be working with and around this vulnerable population. We take plenty of precautions but there is no point in putting anyone in a situation where they are at increased risk if you don’t have to.
In my street clothes and cloth mask today as I was off
Depending on the regulations, how things change, and facility policy, testing may have to happen every 14 days or more (or less???) to ensure we remain safe to work with the geriatric population in these types of facilities. My job is to do no harm, to keep people safe, and to improve their function. Getting tested for COVID-19 is part of that package.
I will be interested to see if and when other settings will mandate COVID-19 testing. I could really see it in the home health arena due to exposure risk and just reassuring patients you are safe to enter their homes if they are self-isolating for health reasons.
UPDATE: My results came back (-)
How was your COVID-19 testing experience? Tell me about it in the comments!
So, who’s up for some bloodwork? Venipuncture, anyone? Finger prick, maybe? No..? Oh… Well, ok then. I’ll carry on. I know it may sound a bit crazy, but as a PT, I actually do some (very) minor blood work. I’m not trained as a nurse or phlebotomist or anything like that. Nope. Just some on-the-job-training…
“Patients exchanging habits of activity for complete rest are likely to become rapidly worse.” This quote fuels my everyday. These words have informed nonsurgical and surgical rehabilitation and its evolution from handing out bed rest like Oprah hands out cars to getting people moving early and keeping them moving often. Here’s the crazy thing: This…
Let’s talk about this super simple technique that can change everything. Diaphragmatic breathing is really just how we are all supposed to be breathing most of the time. The purpose of the diaphragm is to facilitate breathing. Diaphragmatic breathing improves gas exchange and increases lung volumes. These are all really good things if we need to…







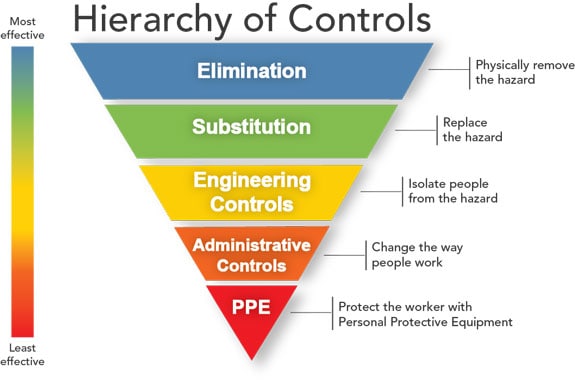









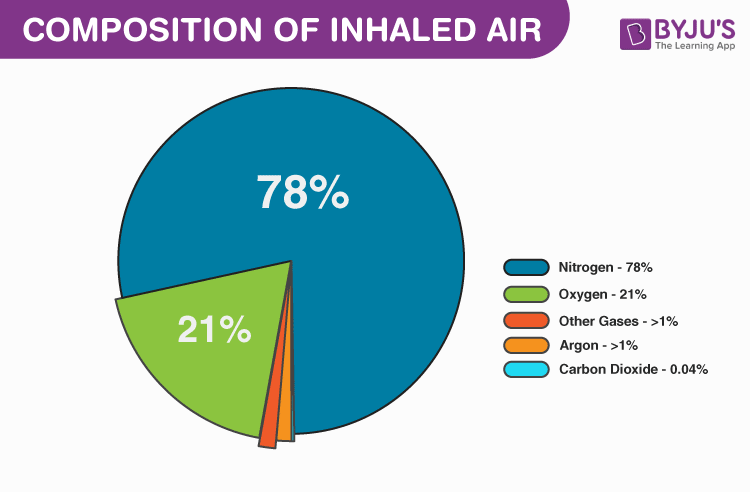


![Buy Oxymizer Disposable Oxygen Conserver [Oxygen Therapy]](https://cdns.webareacontrol.com/prodimages/1000-X-1000/1/r/12520205933Drive-Oxymizer-Disposable-Oxygen-Conserver-L.png)