
Isn’t COVID-19 just a respiratory disease? If only that was true. We are good at treating respiratory infections. We have lots of drugs for viral, bacterial, parasitic, and fungal infections of the lungs. Most of them work really well! We also have several backup treatments, inhaled medications, and adjuvant therapies (like rehab!) that make primary treatments even more effective. We are pretty darn good at treating respiratory infections. So, if COVID-19 was a respiratory disease only, we would have been all over that. We’ve been battling influenza in varying forms for over a century. We’ve stopped pneumonia in its tracks in even the most fragile patients. So, why haven’t we been able to put a cork in COVID-19? The answer is NO, it isn’t just a respiratory disease.
Yes, influenza can give you muscle aches. Yes, pneumonia, if left untreated, can lead to sepsis. But, COVID-19 causes severe physical damage to multiple organs and systems in your body. Particularly susceptible are the kidneys, heart, vasculature, and brain. It is thought that their susceptibility is due to their expression of ACE-2 receptors, something this coronavirus is eager to find. Even the blood-brain barrier can’t keep it out, because this coronavirus destroys the barrier. The pancreas, skin, and blood vessels are also at particular risk.
We’ve talked about these topics quite a bit in several previous posts. What do I have to offer that is new? I’m going to tell you how to start assessing and treating COVID-19 like a multi-system disease. Just like we treat diabetes, just like we treat heart failure, just like we treat most other chronic diseases.
Notice how I mention “chronic” disease? That’s intentional. Many people who didn’t require any medical intervention are several months out now on their infections and are still experiencing symptoms such as shortness of breath with little to no activity, and other symptoms that just keep lingering. Many experts feel that the damage this coronavirus causes to the endothelium (the lining of the vessels) will cause a long-term increased risk for blood clots and strokes. As rehab providers, we need to know if someone has had COVID-19 because we will want to keep this in the back of our minds when performing our differential diagnosis.
Inflammatory markers, including C-reactive protein and interleukin-6, are found in increasing numbers in patients with and after COVID-19 infection. These are the same inflammatory markers we blame for so many long-term inflammatory conditions. Down to the sub-cellular level, this disease changes our physiological function, interfering with the renin-angiotensin-aldosterone system (RAAS). This hormone-based system also helps regulate inflammation, fluid levels, and blood pressure. People who have heart failure depend on regulated fluid levels in their bodies, so upsetting this already debilitated system would cause them serious harm.

Sure, we can treat the inflammation with dexamethosone. We can pump you full of antibiotics to prevent opportunistic infections. We can give you antivirals to slow the damage. We can thin your blood down to water and hope it still carries oxygen. We can treat the breathing problems. Heck, we just can breathe for you. We can put you out so you don’t feel a thing. We can filter your blood for you. We can circulate your blood for you. We can flip you over so you breathe better. We can even wake you up just a little bit and walk you around the room attached to 30 different machines with a team of 8 or more highly skilled medical providers… But my goodness, we’ve never really had to do all of that at one time for one single person… And now we are doing it for thousands of people at hundreds of facilities all over the world.
Even if we come up with the perfect treatment, perfect engineering controls, or preventative tomorrow (fingers crossed!), we still have people currently experiencing COVID-19 and its sequelae that need quality treatment. We can actually predict with greater than 90% accuracy what someone’s clinical disease course will be, what levels of care they will need, and what treatments will be the best for them at each phase. We know that COVID-19 isn’t overall that deadly, but we do know that it is very damaging, and either one isn’t good. Polio was pretty damaging, too. We have many studies confirming airborne transmission, especially in close confines and indoor environments.
All this to say that there is a lot the medical community can do for patients at risk for and with COVID-19. But what can WE, the rehab professionals, do?
Evaluating a Multi-System Disease
If we have a patient with diabetes, we don’t just treat their blood sugar. Even as rehab providers, we look at their circulation, their peripheral sensation, their central and peripheral balance, their cardiac function, their vision, their skin, their shoes, and many other things because we know that diabetes causes impairments in all of these domains. If we have a patient with heart failure, we never just look at their heart, do we? We know they have changes in their kidneys, their lungs, their vasculature, and their muscles… So we use tests and measures to address all of these components. This is exactly How we need to be looking at survivors of COVID-19.
In the rehab world, what can we do to address COVID-19 as a multi-system disease? How does this change the way we screen, evaluate, and treat? You will need to look at the whole patient. Even in the outpatient setting, they are not just knee pain who had COVID-19 two months ago. If you are seeing patients in any setting who have had COVID-19, even tested positive but remained asymptomatic, you need to be looking at a number of things and the APTA has summed it up in 5 easy measures:
- Physical Function. Can we start out with, “Duh?”. The best way to do that is to use the Short Physical Performance Battery (otherwise known as the SPPB). This is a combination of three already standardized tests (timed chair rise, gait speed, and static balance) that give you raw scores and a sum score that is highly predictive of function. This is a great tool across functional levels and gives you a good amount of functional information to inform and direct your treatments. You can get all the deets here:
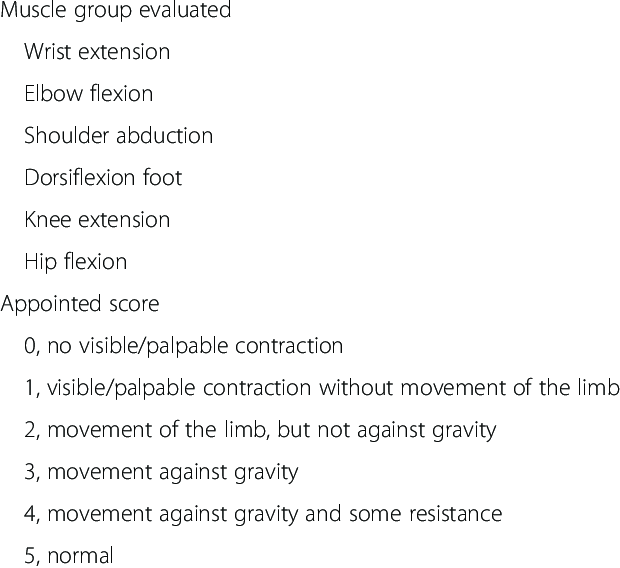
2. Strength. COVID-19 is known for causing weakness in the small muscle groups and the core. You may have a patient who can stand, but they can’t write their name. They may do a squat, but can’t walk 10 feet. Anyone who you meet that has had an ICU stay for COVID-19 is at risk for ICU acquired weakness (ICUAW). In that case, the Medical Research Council Sum Score (MRC-SS) is recommend for assessing strength. There are several articles listen in the references for the MRC-SS, but generally it is a combination of manual muscle tests of certain muscle groups.
Here is the source for this file: ResearchGate.
You can also learn more about scoring this was from this video:
3. Endurance. You’ve probably heard by now of someone who had COVID-19 and needed months of rehab. Or who didn’t go to the hospital but still gets short of breath walking short distances. Whether it’s due to long term immobility in the hospital or actual parenchymal damage to the lung tissue (or other body systems), endurance becomes significantly affected. The recommended test for endurance in people who have had COVID-19 is the 2 minute step test. This is a favorite of mine for people of all ages! I’ve used this for my ESRD patients, VAD patients, young athletes, and middle-aged adults. You can download the one-page here:
4. Cognition. We have talked several times about the effects COVID-19 can have on the brain. In this case, you should probably have a tool in your pocket to assess cognition. There are some specific cases of COVID-19 that are associated with delirium lasting longer than 72 hours. In the absence of other serious symptoms, you may find this patient in your clinic for any number of reasons or you may find that one of your current patients starts to develop some strange symptoms. The SLUMs (the Saint Louis University Mental Status Exam) is the recommended assessment to use in this case. You can access it for free here:
5. Quality of Life. Isn’t this what we should always be focused on? What can we do as rehab providers to improve someone’s quality of life? Unfortunately, we so often do not assess or quantify it, so it can be difficult to demonstrate improvement other than subjective reports. The ED-5Q-5L is a simple questionnaire that can reliably quantify the quality of life for patients who have had COVID-19. Unfortunately, I can’t give you this one. However, you may be able to get it for free when you register with the company that created it. You can do that here: https://euroqol.org/support/how-to-obtain-eq-5d/
Keep Reading HERE for more on Assessments and Interventions for COVID-19!
There is your toolbox! You’ve got something for every major system. Obviously, you can insert other objective measures you may need specific to your patient. Hopefully, soon, we won’t need to worry so much about all of this, but until that day comes, we will continue to be the frontline against community spread, and the treatment for those with long-term medical complications regardless of their setting.
Keep in mind that patients with Long-COVID may not be up for doing some or all of these assessments in one visit, especially if they have post-exertional malaise. Also, you may want to include a few other screenings… More on those topics next week!
Have you used any of these tools for assessing patients with COVID-19 or patients experiencing Long-COVID? Did they paint an accurate picture? Tell me in the comments.
More Reads…

Pressure… Pushing Down On Me…
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…

Dehydration
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease

Chronic Disease Part 3: Urinary Incontinence – Part 1
NEXT FEATURE IN THE CHRONIC DISEASE MANAGEMENT SERIES!!!
Let’s learn how to manage incontinence! But wait, that’s not a chronic disease, is it? Well, let’s take a look and find out!
References:
American Physical Therapy Association. (2020). APTA Academies and Sections Consensus Statement: COVID-19 Core Outcome Measures. Retrieved from https://www.apta.org/contentassets/1a6e0ee7cd25403888d2959c1c8476cd/covid-19-core-outcome-consensus-statement-june-2020.pdf
Arshad, S., Kilgore, P., Chaudhry, Z. S., Jacobsen, G., Wang, D. D., Huitsing, K., Brar, I., Alangaden, G. J., Ramesh, M. S., McKinnon, J. E., O’Neill, W., Zervos, M., & Henry Ford COVID-19 Task Force (2020). Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalized with COVID-19. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases, 97, 396–403. https://doi.org/10.1016/j.ijid.2020.06.099
Azimi, P., Keshavarz, Z., Laurent, J. G. C., Stephens, B. R., Allen, J. G. (2020). Mechanistic Transmission Modeling of COVID-19 on the Diamond Princess Cruise Ship Demonstrates the Importance of Aerosol Transmission. medRxiv 2020.07.13.20153049. Retrieved from doi: https://doi.org/10.1101/2020.07.13.20153049
Bonn, D., Smith, S. H., Somsen, A., van Rijn, C., Kooij, S., van der Hoek, L., Bem, R A. (2020). Probability of aerosol transmission of SARS-CoV-2. medRxiv 2020.07.16.20155572. Retrieved from doi: https://doi.org/10.1101/2020.07.16.20155572
Connolly, B., Thompson, A., Moxham, J., Hart, N. (2020). Relationship Of Medical Research Council Sum-Score With Physical Function In Patients Post Critical Illness. American Journal of Respiratory and Critical Care Medicine. 201:A3075. Retrieved from https://doi.org/10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A3075
Connolly, B. A., Jones, G. D., Curtis, A. A., Murphy, P. B., Douiri, A., Hopkinson, N. S., Polkey, M. I., Moxham, J., & Hart, N. (2013). Clinical predictive value of manual muscle strength testing during critical illness: an observational cohort study. Critical care (London, England), 17(5), R229. https://doi.org/10.1186/cc13052
Kingsland, J. & Sanfins, A. (2020). COVID-19: Doctors round up evidence of damage outside the lungs. Medical News Today. Retrieved from https://www.medicalnewstoday.com/articles/covid-19-doctors-round-up-evidence-of-damage-outside-the-lungs
Rikli, R.E., Jones, C.J. (1999). Functional fitness normative scores for community residing older adults ages 60-94. Journal of Aging and Physical Activity. 7:160-179. https://geriatrictoolkit.missouri.edu/cv/2min-step-rikli-jones.doc
Santarpia, J. L., Herrera, V. L., Rivera, D. N., Ratnesar-Shumate, S., Reid, S., Denton, P. W., Martens, J. W. S., Fang, Y., Conoan, N., Callahan, M. V., Lawler, J. V., Brett-Major, D M., Lowe, J. J. (2020). The Infectious Nature of Patient-Generated SARS-CoV-2 Aerosol. medRxiv 2020.07.13.20041632. Retrieved from doi: https://doi.org/10.1101/2020.07.13.20041632
Tsui, E. L. H., Lui, C., Woo, P. P. S., Cheung, A. T. L., Lam, K. W., Tang, T. W. , Yiu, C. F., Wan. C. H., Lee, L. H. Y. (2020). Development of a data-driven COVID-19 prognostication tool to inform triage and step-down care for hospitalised patients in Hong Kong: A population based cohort study. medRxiv. 2020.07.13.20152348 Retrieved from doi: https://doi.org/10.1101/2020.07.13.20152348

Follow @DoctorBthePT on Twitter for regular updates!

{kind=link}
3 thoughts on “More Than Just A Respiratory Disease: The COVID-19 Toolbox”