
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they breathe. My guess is that your patients have this in common with my patients, even if you are in an outpatient orthopedic clinic, or a skilled nursing facility, or a pediatric rehab hospital. So it goes without saying that one of the main interventions I provide for all of my patients in proper breathing to promote physiological function and mobility. I base many of these interventions on the regulation of intra-abdominal pressure. I had no idea how broad this topic would become once I got started!
Intra-abdominal pressure is a huge factor in many disease states, post surgery, and with impaired mobility. If I can regulate someone’s intra-abdominal pressure, odds are I can help them breathe better, move better, reduce their pain, and even make it to the bathroom on time. Why is that? Because that pressure inside your abdomen pushes on everything else in there and elsewhere! These changing pressure dynamics are really important for digestion, breathing, posture, urination, circulation, neurological function and hemodynamic stability. Don’t believe me? Ask Mary Massery! She will tell you all about it! Normal Intra-abomdinal pressure at rest ranges from 13-20 mmHg depending on the position (supine vs sitting vs standing). When you jump or cough, that pressure can go as high as 171 mmHg in young healthy people.

If you work on the opposite end of the spectrum of patients from me (i.e. the super fit, young, healthy folks) then you might try to regulate intra-abdominal pressures in your athletes for very specific reasons. Weightlifters and powerlifters tend to utilize intra-abdominal pressure to brace when they lift very heavy loads. Techniques vary, but using that pressure and the braces they wear around their abdomen, they can push out a large amount of power. However, lifters also tend to suffer some of the side-effects of using intra-abdominal pressure such as urinary or fecal incontinence, aneurysms, and blood pressure issues. Strangely enough, these are some of the exact same things post-partum women experience and for exactly the same reasons. Intra-abdominal pressure is used to push babies out, too! Let’s dig in to those a bit more.
Who Has Increased Intra-Abdominal Pressure?
The number one reason I work on intra-abdominal pressure is far and away to reduce urinary incontinence. Think about it. All that pressure inside your abdomen pushing down on… your bladder! The standard method for measuring intra-abdominal pressure is actually to measure it through the bladder! Your bladder can only take so much and eventually won’t stand to the pressure and it will let go. This is called stress urinary incontinence and 80% of women and 45% of men will experience this at some point in their life. In addition to incontinence, this pressure can also cause over-lengthening of the ligaments that hold your organs in place. This can result in herniation of the organs through the abdominal wall (I’m sure you’ve seen plenty of these) or prolapse of the pelvic organs. All things that we ABSOLUTELY DO NOT WANT.
The pelvic floor muscles can normally accommodate to this pressure for short periods of time, but sustained pressure or large amounts of pressure will eventually cause the pelvic floor muscles to either fatigue or lengthen beyond their ability to efficiently contract. After these events, the amount of intra-abdominal pressure that causes incontinence episodes becomes less and less and herniations and prolapses increase more and more. You may be thinking that this is important for post-partum women, but intra-abdominal pressure regulation is also incredibly important for people who have COPD, Heart Failure, Obesity, Cirrhosis, neurologic conditions, and a host of other chronic diseases. That’s because all of these diseases cause changes to intra-abdominal pressure in some way.

For COPD, these patients are coughing frequently. This repeated coughing causes sustained stresses on the pelvic floor muscles and the increased lung volume in obstructive lung diseases increases the pressure within the abdomen. For heart failure, the increased amount of fluid accumulated leads to increased pressure in the abdomen, especially if they experience ascites (accumulation of fluid in the abdomen). Obesity also leads to increased intra-abdominal pressure as the build up of fatty tissue within in the organs takes up space, therefore increasing pressure. With cirrhosis, the liver increases in size due to one of many possible reasons such as edema or fat build up. This takes up extra space in the abdomen, increasing the overall pressure. Tumors or other space-occupying lesions in the abdomen create the same effect. Neurologic conditions can result from increased intra-abdominal pressure, but can also create changes in intra-abdominal pressure. And then, people can have more than one of these conditions and every additional breath can become a turn of the vice. All of these things are becoming so much more common that abdominal hypertension has become a typical diagnosis that can lead to severe health conditions.
Why Do We Need to Regulate Intra-Abdominal Pressure?
Pulmonary conditions are front and center right now thanks to the global COVID-19 pandemic, we will start there. There have actually been cases documented of compression atelectasis (too much fluid in the abdomen increasing pressure so high that the lungs have no where to expand) causing multi-system organ failure. Compression to this level, although somewhat rare, causes internal organ compression to the point of ischemia. This means that all the organ systems can’t get blood because the blood pressure cannot overcome the intra-abdominal internal pressure. As Physical Therapists, we are pretty familiar with compartment syndromes, so to compare, this condition is also known as abdominal compartment syndrome. You can imagine that the intestines, kidneys, and pretty much everything else in the abdominal compartment doesn’t fare well under these conditions. Abdominal compartment syndrome can also be a complication of child delivery.
Returning to our post-partum patients, women who have Cesarean sections (C-sections) need to reduce intra-abdominal pressure when they move to reduce strain on their incision or surgical work. This is also true for most people who have had any kind of abdominal surgery such as hysterectomies, laparatomies, laparascopies, and trachelectomies, and several spinal surgeries such as decompressions, fusions, etc. I’ve also found reducing intra-abdominal pressure to be extremely helpful for people who have had new colostomy placements, as they have decreased pain with movement and decreased complications with their colostomies. We will go in to more detail on all of this later.
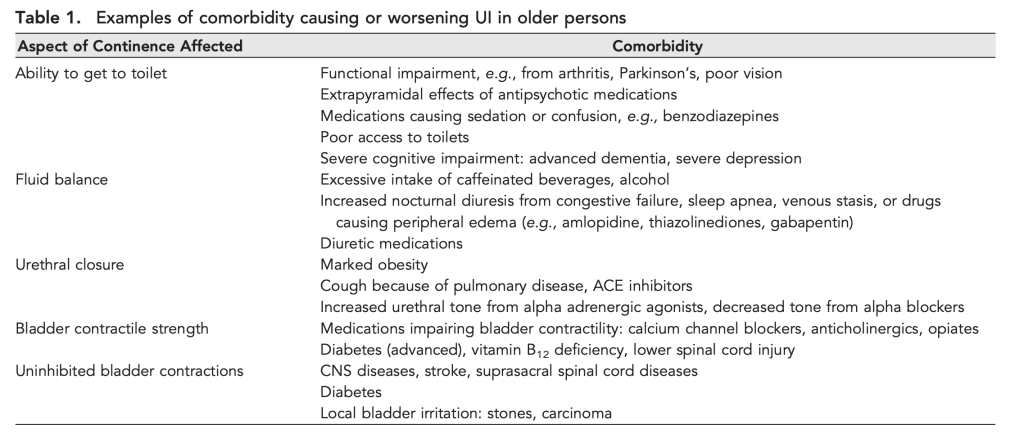
Reducing intra-abdominal pressures is crucial in patients with chronic health conditions such as COPD, heart failure, cirrhosis, obesity, and many others. Why, you might ask? They don’t have surgical incisions or internal work that they pressure is pushing on, so what can we do. I’ll take you back to the very first word of this post. You can help them BREATHE. You are essentially providing interventions to improve V/Q matching, because you are allowing increased ability to ventilate and, therefore, increasing potential to diffuse and perfuse. In addition to breathing, most of these patients also experience some kind of incontinence. This is, in large part, due to the increased intra-abdominal pressures, but also due to the effects of medications and altered fluid dynamics. You can’t change the medications or disease, so change the pressure.

The neurological population (which we will discuss more in a bit) also struggles with increased intra-abdominal pressures. We will dive deep into the neurologic mechanisms by which this effects the body, but increased intra-abdominal pressure actually impairs the flow of cerebrospinal fluid in the central nervous system. These pressures can also increase venous distension which puts direct back-pressure on the eyes and optic nerve. All of the major neurological components of function are negatively impacted by high intra-abdominal pressure.
Do I Always Want to Reduce the Pressure?
Well, no. Just like everything else in the medical world, nothing is ever “always.” Even lab values that are “not compatible with life” can still be seen in calm living individuals. So, no, you don’t always want to reduce intra-abdominal pressure. In fact, sometimes you want to increase it!
For patients who have medical conditions like Parkinson’s Orthostasis, Postural Orthostatic Hypotensive Syndrome (POTS), or even just your standard orthostatic hypotension, you actually want to INCREASE intra-abdominal pressures, at least temporarily. We achieve this in the short term by actually instructing patients to hold their breath during an activity. This places pressure on their internal vasculature, holding blood up into their brain when gravity says otherwise (like with orthostatic hypotenison: when the patient goes up, their blood – and blood pressure – go down), which can help reduce symptoms of dizziness or blacking out. Obviously we have to let them breathe and return intra-abdominal pressure to normal eventually but we hope to get them active enough to keep the pressure up (usually with some exercise). In the long term, we can use devices like abdominal binders and compression garments to increase the pressure.
For post-partum patients, abdominal binders are also frequently used. This can be for several reasons, but you may actually want to increase their intra-abdominal pressure to apply compression to reduce internal bleeding (there can be a lot of bleeding with and after birth). It is also documented that intra-abdominal pressure can elevate significantly even in healthy pregnancies. This should seem obvious because there is a human growing in a limited space so the pressure has to go somewhere. But, because this is a slow process, pregnant patients tend to accommodate to this pressure over time. However, that tiny human and all it’s stuff leaves the abdomen quickly, which is a harder process to accommodate to. Birth also creates a large fluid deficit which can leave a post-partum patient a bit hemodynamically unsteady. These factors cause the intra-abdominal pressure to drop and some patients may need some pressure support for a while to return to activities normally.

Other conditions that cause significant fluctuations in hemodynamic stability, such as severe burns, dehydration, mid-brain injuries, and multi-traumas may also require pressure support for some time.
The Valsalva Maneuver
Some people try to increase their intra-abdominal pressure intentionally on their own. This is typically done using a Valsalva maneuver, or “bearing down”. People use this to place intentional pressure on their organs to achieve a certain goal. This may be to push a baby out, to defecate, or to stabilize their spine. However, using a Valsalva maneuver too often or several times in a row can lead to vasovagal syncope. We mentioned the vagus nerve above and you can see in the drawings below that it provides innervation to the vasculature of the abdomen. Put too much pressure on the vasculature of the abdomen (aka the abdominal aorta) and you will lose pressure support for the blood flow to your brain and you’ll faint. The mechanism also may occur from that pressure causing overstimulation of the sympathetic nervous system resulting in a severe “faint” response, which is your body’s only way of forcing you to stop producing the pressure. It’s basically a safety mechanism to prevent abdominal compartment syndrome.
Alone, vasovagal syncope isn’t dangerous and is usually self-limiting. Just like when you hold you breath long enough, your body will force you to breathe somehow, even if it’s by making you pass out so that you breathe again. However, it’s what happens after you pass out that concerns us. I’ve treated several patients for head injuries, wounds, and broken bones secondary to the fall they experienced during their syncopal episode.
Valsalva Maneuvers are not a great solution to pelvic organ function. This increased pressure to go to alleviate constipation is not effective and has significant side effects. If you are in need of better options, please check out the post on Incontinence Management – Coming Soon!
So What Do I Do To Help These Patients Breathe?
Thankfully, that’s the easy part! Odds are, you already know this, you just may not know the deeper “why” behind why you do it or how to widely apply it. I’m sure you are constantly telling your patients to breathe during their exercises. And I’m sure they repeatedly hold their breath. Mine do! Which tells us they are attempting to stabilize and produce force improperly, i.e. not using their muscles.
If you read my post on pursed lip breathing, I told you a little bit about this. In that post we talked about how pursed lip breathing, when done correctly, can stimulate the parasympathetic nervous system to reduce anxiety and calm the sympathetic responses. I just used this with a patient recovering from COVID-19 very successfully. When she started to get short of breath and panic, we regulated her breathing and her oxygen saturation sprang right back up. But regulating breathing by changing intra-abdominal pressures can help with so much more! I’m going to take you back to the basics of what you know.

The reason behind this effect is the change in intra-abdominal pressure which changes forces and stimulations to the sympathetic trunks within the abdomen. Applying our anatomy knowledge, we can picture that. Remember the sympathetic trunks from all those years ago? They are coming back. Look at those abdominal sympathetic trunks! They are all over the length of the spinal column from the diaphragm to the pelvic floor and there are more throughout the length of the spine. They feel EVERY change in intra-abdominal pressure and they respond to it. They feel the pressure, they get stimulated and they set off the fight, flight, or faint responses, because that’s their job! Most of the time, we see this manifested as the patient getting anxious, worked up, angry, or refusing to participate. We can also see increased pain or fainting (like we talked about above).

So, by reducing the pressure, thereby reducing the stimulation on the sympathetic nervous system, we calm the fight, flight, or faint response mechanisms. Like we talked about in the post on pursed lip breathing, we also then engage the parasympathetic systems. The parasympathetics mostly branch from Cranial Nerve X: The Vagus Nerve. The remainder of the parasympathetics come from the sacral trunks. Reduce strain on the pelvic floor, and the parasympathetics can do their job.
And, don’t forget, you aren’t just utilizing the autonomic functions to regulate breathing, you are also increasing space for the lungs to expand. This increases the potential for vital capacity, increases the space for residual volume, and reduces the required PEEP, meaning you will have more patent airways. Increased intra-abdominal pressures actually start to require a higher than normal PEEP (positive end-expiratory pressure) to maintain patent airways. Eventually, the body can’t create a high enough natural PEEP to keep breathing properly. Reducing intra-abdominal pressure increases the available space for lung expansion with inhalation, reducing the effort and increasing the efficiency of breathing, and reducing the required PEEP. Significant improvements are noted on Pulmonary Function Tests (PFTs) including improved FEV1 and improved FRC, both markers of overall pulmonary function, when intra-abdominal pressure is reduced.
How Can I Reduce the Pressure So These Patients Can Breathe and Move Better?
After spine or abdominal surgery or birth, patients are NOT taught how to move! They strain. They hold their breath. They endure. Or they don’t move at all. Patients who have chronic diseases have been slowly accommodating to increased intra-abdominal pressure and changes in lung volumes and compliance over time, so may not feel an acute change in their symptoms. But, all of this is 100% avoidable. And, oh so simple. This is where you come in.
If your patient is having pain with movement post-operatively, go to your basic techniques and then we will build on them a bit. We know for post-operative spine patients, log rolling is very important to prevent them from breaking their movement and positioning precautions, but this concept can be applied broadly. Especially for patients who have abdominal incisions, we need to decrease the tissue strain or they are going to hold their breath because of pain. Then, we have to pair breathing with the movement to reduce sympathetic activation and reduce intra-abdominal pressure so that muscles can function properly with an appropriate vitals response. Here are the steps for something simple:
Getting out of bed
- Start in Supine (lowest intra-abdominal pressure)
- As they breathe out: Slide one foot up the bed while breathing out through the whole motion, breathe in
- As they breathe out: Slide the other foot up the bed while breathing out through the whole motion (this brings you to hooklying), breathe in
- As they breathe out: As a whole unit, roll on to one side while breathing out through the whole motion, breathe in
- Patient may need to use grab bars, trapeze, bed rails, drop knees to the side, UE support from you, or momentum from swinging UEs
- From sidelying, position hands near head and shoulder on bed to push up to sitting and bring feet forward over edge of bed while breathing out
- With or without assistance, push up from the arms and drop feet downward to the floor while breathing out through the whole motion (this achieves sitting which created only small increases in intra-abdominal pressure in comparison to supine).
I know that seems like a lot of steps, but it moves rather fluidly once you teach it. It is so important to break the task down and ensure the patient moves slowly and breathes out (exhales) with each position change. This reduces the intra-abdominal pressure during movement, keeps tissue strain to a minimum, and also keeps that sympathetic nervous system quiet so the patient can focus on moving. If your patient uses supplemental oxygen, make sure they are breathing in through their nose so they can utilize it most effectively to maintain V/Q matching. And, even though this is a lot of steps which increases the time required to perform this activity, your patient will thank you for the increase in their comfort. They won’t have to do it this way forever, just until they recover from their surgery.
Now you can take these concepts and apply them widely, like with sitting down on the toilet, or getting up from the floor, or with performing their exercises in the gym like their next plyo task or weighted deadlift. If your patient experiences pain or difficulty breathing with movement, you’ll likely see a decrease in either or both symptoms because of those mechanisms we discussed above. In the post-partum population, you may find that your patient needs both pressure support and pressure reduction depending on the movement task.
If you are using intra-abdominal pressure regulation to help treat your patients with stress incontinence, there are some specific ways you need to build breathing in to you exercises and other treatments. Remember how we talked about the pressure this places on the pelvic floor? Yea, you have to reduce that pressure if you want your patient to have the proper length-tension relationships in their pelvic floor muscles to even attempt a proper muscle contraction. It is so often that people hold their breath while performing pelvic floor exercises. I like to tell my patients that those particular muscles are NOT breathing muscles. They laugh, which then means they are breathing, which makes me happy, and then we try again. I think that leads me to my next post on incontinence management… See you there!
Even if you already knew about these interventions, I’m hoping that you now can better utilize them for a wider variety of patients. I also hope you have a really good understanding of WHY you use these techniques. How do you use intra-abdominal pressure regulation in your patients? Tell me in the comments!
Follow my blog for more!
More Reads…

Pressure… Pushing Down On Me…
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…

Dehydration
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease

Chronic Disease Part 3: Urinary Incontinence – Part 1
NEXT FEATURE IN THE CHRONIC DISEASE MANAGEMENT SERIES!!!
Let’s learn how to manage incontinence! But wait, that’s not a chronic disease, is it? Well, let’s take a look and find out!
Cobb, W.S., Burns, J.M., Kercher, K.W., Matthews, B.D., Norton, H.J., Heniford, B.T. (2005)
Normal Intraabdominal Pressure in Healthy Adults. Journal of Surgical Research. 129(2):231-235. https://doi.org/10.1016/j.jss.2005.06.015.
Depauw, Paul & Groen, Rob & Van Loon, Johannes & Peul, Wilco & Malbrain, Manu & De Waele, Jan. (2019). The significance of intra-abdominal pressure in neurosurgery and neurological diseases: a narrative review and a conceptual proposal. Acta Neurochirurgica. 161. 1-10. 10.1007/s00701-019-03868-7.
Frezza, E.E., Shebani, K.O., Robertson, J. et al. Morbid Obesity Causes Chronic Increase of Intraabdominal Pressure. Dig Dis Sci 52, 1038–1041 (2007). https://doi.org/10.1007/s10620-006-9203-4
Mayo Clinic. (2021). Vasovagal Syncope. Retrieved from https://www.mayoclinic.org/diseases-conditions/vasovagal-syncope/symptoms-causes/syc-20350527#:~:text=Vasovagal%20syncope%20(vay%2Dzoh%2D,blood%20pressure%20to%20drop%20suddenly.
Sugerman, H.J., Bloomfield, G.L. & Saggi, B.W. Multisystem organ failure secondary to increased intraabdominal pressure. Infection 27, 61–66 (1999). https://doi.org/10.1007/BF02565176

Follow @DoctorBthePT on Twitter for regular updates!

















































































{kind=link}
{kind=link}