
This is part 2 in a multi-part series on the role of Rehab Providers in the management of chronic disease. Don’t forget to check out Part 1: Heart Failure!
Chronic Obstructive Pulmonary Disease is a widely diagnosed disease of the lungs that includes the diagnoses of emphysema and chronic bronchitis. COPD can be caused by several things such as genetic diseases (alpha-1-antitrypsin deficiency, for example, which causes emphysema in children and adults), lifestyle choices (such as smoking), work environments with poor engineering controls and toxic output (asbestos, coal, and steel production), or community/home environments that require regular burning of substances with toxic output for a heat source or for food preparation.
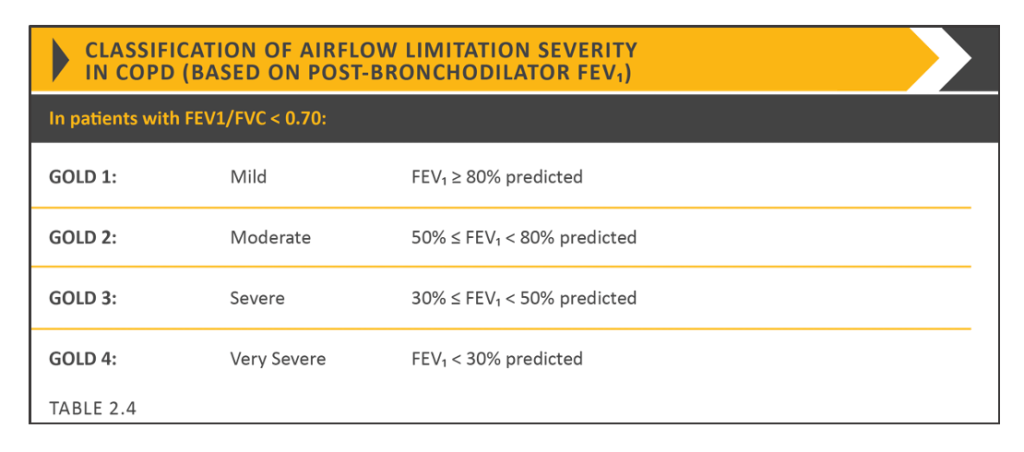
Like the name suggests, it is an obstructive lung condition, meaning that stuff gets in the airway making it hard for air to get OUT of the lungs. Air trapping, mucus hypersecretion, physiological and physical changes to the body, chronic cough, and decreased overall activity level are all signature components of COPD. COPD used to be ranked based on severity for GOLD levels which are based on FEV1. This system is not part of a clinical picture of symptoms assessment instead of the sole descriptor:
COPD is often accompanied by (or even caused by) other chronic diseases such as left heart failure. It can exist in isolation, but even then, the treatments tend to induce other chronic conditions. Long term COPD management with corticosteroids has a host of side effects including osteoporosis, diabetes, vision impairments, and increased risk of infection (among others). Long term use of bronchodilators (inhalant medications, typically) have been linked to myocardial infarctions, hypokalemia, and bronchospasm. These side effects lead to some interventions being contraindicated (such as percussion) that would otherwise be helpful in COPD symptom management.
If you treat patients with COPD regularly, you tend to get a feeling for what COPD looks like. That’s because it comes with physiologic changes that eventually result in physical changes (similar to most chronic diseases!) that can be spotted across the room: barrel chests, blue-ish lips, digital clubbing, sunken eyes, coughing regularly, accessory musculature popping out of the collar of a shirt… And those are just the things we can see. The thinks we can’t see are worse. Chronic cough is also associated with urinary incontinence and chronic back pain, and diseases of breathing are associated with depression and anxiety.
Our goal with patients who have COPD is two-fold:
Reduce the risk of rehospitalization and improve quality of life.
These two goals include all the medical management and functional interventions we would apply. But first…
We have to quantify it
Just because someone has COPD doesn’t mean they necessarily need a PT or any other rehab provider involved in their care, so we need to make it clear when and why we are necessary. We need to express what deficits they are facing because of their COPD (or any other comorbidity). You’ll need some tools for this. There are many that are somewhat generic, but there are some disease specific tools, too. These tools are great because they can really help direct your interventions to give the patient the most BANG for their BUCK! We will talk about a few of them here, but there are many.
The COPD Assessment TEST (CAT) – highly recommended and free, this is the test recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD)
Leicester Cough Questionnaire (LCQ) – Used frequently in research specific to COPD
Chronic Respiratory Questionnaire (CRQ) – proprietary assessment owned by McMaster University
SF-36 – More generic but a wealth of evidence to support its applicability (developed at RAND as part of the Medical Outcomes Study)
The Cough and Sputum Assessment Questionnaire (CASA-Q) – also proprietary, but validated with the SF-36 and disease specific
The Patient Reported Outcomes Measure Information System (PROMIS) Global Rating Scale – a free NIH funded HRQoL Questionnaire
Many physical function and exercise capacity tests can also be utilized, such as the 6-minute walk test, the 2-minute step test, the 400 meter walk test, and many others. For more information on standardized tests and measures that are valid for patients with COPD, check out SRALab (formerly rehabmeasures.com). I like to use a combination of different measures to better capture the “whole-patient” picture, one physical, one subjective report, and maybe one or two others based on the reported deficits.
Then we have to treat it
You may find several areas of impairment based on your chosen outcomes measures, so you may have several areas of physical, mental, and emotional function to address, either by yourself or in conjunction with your team. Chronic diseases like COPD, which deplete oxygen supply to the brain and weigh a heavy burden on patients and their caregivers, tend to have long lasting emotional and mental effects, so don’t forget to refer to your colleagues across disciplines.
For people with COPD, secretion management is also going to be a large part of their long term plan, but it is also something they face acutely in the hospital or subacute setting that rehab therapists can very easily improve. We know that, independent of any other factors, mucus hypersecretion is a risk factor for hospitalization and death. So what do we have in our toolbox? Oh, so many great things! Click the links for more details of each tool or technique.

Oscillatory PEP therapy is effective at increasing secretion transport, decreasing breathlessness, reduced hyperinflation, and is as effective as other airway clearance techniques at improving disease-specific quality of life. However, flutter valves have ben found to be more fatiguing for patients than other types of airway clearance such as the active cycle of breathing (ACBT). Patients with COPD do not experience greater discomfort when performing one airway clearance technique over the other, even when utilizing gravity-assisted positions (or postural drainage). ACBT and oscillatory PEP have near equal outcomes for patients with COPD when performed with or without postural drainage positions when it comes to dyspnea, cough frequency, and overall weakness. Although, ACBT was found to be more efficient as moving secretions from the smaller focal airways than oscillatory PEP interventions. There were also no differences in the effects on lung function as both tools improved FEV1 and FVC. In my mind, that’s great news!
That means we can utilize either one, depending on our goals with the patient, and still achieve similar outcomes! If our patient fatigues easily, we may stick to the ACBT, but if we are targetting dynamic hyperinflation or need to significantly improve overall quality of life we may chose a PEP. In my regular practice, I give both and here’s why:
- PEP devices are easier to use, remember to use, and take less time to perform than the ACBT.
- Having a PEP around provides a visual reminder that the patient needs to do airway clearance techniques
- I want the effects of both when I treat patients with COPD, as many patients need to improve their disease-specific quality of life and their dynamic hyperinflation, but also fatigue quickly, and I want them to have options. Having options for long term management that can all be performed independently with or without devices increases the chance they will actually be used.
No technique for airway clearance is as effective on its own as it is when combined with something else. Postural drainage can be combined with most techniques to target specific segments.
Then we have to manage it
In addition to secretion management, patients with COPD tend to need supplemental oxygen. There is a high degree of training that is required for the effective use of this drug including how to manage the equipment, how to therapeutically manage the drug from a rehabilitation perspective, and how to incorporate the equipment and the drug in to everyday life. There are many safety concerns that accompany supplemental oxygen delivery, which are usually the reasons rehabilitation providers are brought in. However, if we can prevent the safety events from happening at all by seeing the patient earlier, rather than later, that’s all the better. You can click the links for more information on each piece of this, but I’ll address some of the safety concerns in brief:
- Supplemental oxygen is typically delivered by a static concentrator that utilizes lengths of tubing the deliver oxygen to the patient wherever they are, which means tubing laying on the floor.
- Oxygen needs to be mobile to go with the patient when they go where a large static concentrator cannot follow. Therapists need to facilitate equipment setup to achieve this via mobile concentrators or other portable devices. This equipment must also be coordinated with their assistive device if they have one.
- Backup oxygen supply is essential should there be an interruption in the power supply or the concentrator malfunctions. All patients on supplemental oxygen should have a kilo tank or other backup supply available and know how to access it.
- Patients need to be educated on how to properly store tanks and swap regulators, as well as how to utilize their oxygen through any other delivery device such as their CPAP, a Duet, or a nebulizer.
- Patients need to be educated on when to clean or replace canulas, tubing, masks, connectors, and any other parts of their oxygen delivery system to prevent pneumonia.
I could really just keep going on this forever… I’ve spent a large amount of time teaching patients how to properly use, manage, and maintain their supplemental oxygen. Maybe I’ll just do a whole other post on factors to consider when managing supplemental oxygen. Keep your eyes peeled for that!

Also, keep in mind the long term changes that happen over time with COPD. We need to be keeping our eyes on those ABGs and looking for an elevated PaCO2 which might tell us that our patient has become a CO2 retainer. This is critical in the management of our patients with COPD and will inform how you manage and monitor their oxygen. Click the link to read more. We may also need to strongly promote fall prevention strategies as these patients have a high risk of falls and a high risk of injury with falls. We will talk a little bit more about this later.
Speaking of long term changes, even though we’ve talked this whole time about getting all that trapped air out, we need to briefly talk about getting air in. Specifically, long term diaphragm weakness is to be expected with physical changes like becoming barrel chested. Diaphragm strengthening using an IMT is crucial, but to be used with caution.
Finally, we need to exercise them!
Finally, right? I bet you thought this part would never come. There is currently no Clinical Practice Guideline for Physical Therapists in the Management of COPD (I checked, twice, and emailed people), but the evidence for high-intensity interval training (HIIT) is pretty clear.
High-intensity interval training produces significant increases in maximal exercise capacity based on outcomes of the 6 minute walk test, as well as a reduction in lower extremity discomfort during exercise, which may be due to peripheral muscle changes in response to exercise. Patients with COPD who perform high-intensity interval training respond with an improvement in VO2max that is two to three times greater than with typical moderate intensity training. High-intensity interval training is also known to produce physiological changes including left ventricular remodeling that improves the overall patient response to exercise with increased oxygenated blood traveling to the muscles and other tissues. HIIT also produces improvement in functional activity and exercise capacity (measured via the 6 minute walk test), improvement in lung function (such as FVC), and in work efficiency.
The overall consensus on HIIT for patients with COPD is that, in the end, the outcomes are the same as when using moderate intensity continuous exercise, however, the results are achieved much faster and patient compliance is higher. So High-Intensity Interval Training is how you give your patients more BANG for their BUCK.
If you are not a provider in a pulmonary rehab setting, do NOT forget about pulmonary rehab! Evidence has shown that pulmonary rehab programs result in 52% fewer hospital readmissions, 4.27 less days in the hospital, and 19% fewer deaths in the same time frame in comparison to patients with COPD who did not have pulmonary rehab!

Of course, HIIT, if designed properly, can be performed by almost any patient at any level. I can absolutely make a HIIT program out of breathing exercises. I’ve done it. So if you have no arms and legs, I can give you a HIIT program. But this cannot be done alone. Address those functional deficits, retrain breathing patterns, improve ADL performance efficiency, and ensure oxygen safety. Manage the medications and their side effects, monitor the oxygen and exertion levels, and instill confidence that COPD may be life-altering, but it doesn’t have to be life-ending.
With chronic disease, it’s a package deal.
What specialty referrals do you make for your patients with COPD? Tell me about them in the comments!
More from the Pulmonary Rehab Toolbox…

Airway Clearance Techniques
SAVED THE BEST FOR LAST! COPD Management bonus content is here and it’s a special treat fo you!

Pulse Oximetry and O2 Saturation
SO MUCH BONUS CONTENT! One of my favorite posts on COPD management – Let’s go for a ride down the river…

Spilling the Box of Pearls: All the Tips on Supplemental Oxygen Management
Can’t get enough BONUS CONTENT! Still managing COPD but struggle with the oxygen? I’ve got you…
Something went wrong. Please refresh the page and/or try again.
References:
Adolfo, J. R., Dhein, W., & Sbruzzi, G. (2019). Intensity of physical exercise and its effect on functional capacity in COPD: systematic review and meta-analysis. Jornal Brasileiro de Pneumologia, 45(6), e20180011. Epub September 26, 2019.https://doi.org/10.1590/1806-3713/e20180011
Birring SS, Prudon B, Carr AJ, et alDevelopment of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ)Thorax 2003;58:339-343.
Chakravorty, I., Chahal, K., & Austin, G. (2011). A pilot study of the impact of high-frequency chest wall oscillation in chronic obstructive pulmonary disease patients with mucus hypersecretion. International journal of chronic obstructive pulmonary disease, 6, 693–699. https://doi.org/10.2147/COPD.S22896
D’Abrosca, F., Garabelli, B., Savio, G., Barison, A., Appendini, L., Oliveira, L., Baiardi, P., & Balbi, B. (2017). Comparing airways clearance techniques in chronic obstructive pulmonary disease and bronchiectasis: positive expiratory pressure or temporary positive expiratory pressure? A retrospective study. Brazilian journal of physical therapy, 21(1), 15–23. https://doi.org/10.1016/j.bjpt.2016.12.001
Global Initiative for Chronic Obstructive Lung Disease (GOLD) (2020). Global Strategy for the Diagnosis, Management, and Prevention of COPD – 2018 Report. [Adobe Acrobat document]. Available from: https://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf
Katajisto, M., & Laitinen, T. (2017). Estimating the effectiveness of pulmonary rehabilitation for COPD exacerbations: reduction of hospital inpatient days during the following year. International journal of chronic obstructive pulmonary disease, 12, 2763–2769. https://doi.org/10.2147/COPD.S144571
Lee, A. L., Burge, A. T., & Holland, A. E. (2017). Positive expiratory pressure therapy versus other airway clearance techniques for bronchiectasis. The Cochrane database of systematic reviews, 9(9), CD011699. https://doi.org/10.1002/14651858.CD011699.pub2
O’Donnell A. E. (2018). Medical management of bronchiectasis. Journal of thoracic disease, 10(Suppl 28), S3428–S3435. https://doi.org/10.21037/jtd.2018.09.39
Rand Healthcare. (2020). The 36-Item Short Form Survey. Retrieved from https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form.html
Ries, A. L., Bauldoff, G. S., Carlin, B. W., Casaburi, R., Emery, C. F., Mahler, D. A., Make, B., Rochester, C. L., Zuwallack, R., & Herrerias, C. (2007). Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical Practice Guidelines. Chest, 131(5 Suppl), 4S–42S. https://doi.org/10.1378/chest.06-2418
Ross, L. M., Porter, R. R., & Durstine, J. L. (2016). High-intensity interval training (HIIT) for patients with chronic diseases. Journal of Sport and Health Science. 5(2):139-144. Retrieved from https://www.sciencedirect.com/science/article/pii/S2095254616300102
Ryrsø, C.K., Godtfredsen, N.S., Kofod, L.M. et al. (2018). Lower mortality after early supervised pulmonary rehabilitation following COPD-exacerbations: a systematic review and meta-analysis. BMC Pulm Med. 18,154. https://doi.org/10.1186/s12890-018-0718-1
Shen, Y., Huang, S., Kang, J., Lin, J., Lai, K., Sun, Y., Xiao, W., Yang, L., Yao, W., Cai, S., Huang, K., & Wen, F. (2018). Management of airway mucus hypersecretion in chronic airway inflammatory disease: Chinese expert consensus (English edition). International journal of chronic obstructive pulmonary disease, 13, 399–407. https://doi.org/10.2147/COPD.S144312

Follow @DoctorBthePT on Twitter for regular updates!

{kind=link}
23 thoughts on “Chronic Disease Part 2: Chronic Obstructive Pulmonary Disease (COPD)”