If you read my post on airway clearance techniques, you probably saw vibration and percussion down at the bottom of the force progression. Although I have covered several other pieces of the force progression (Active Cycle of Breathing, PEP Devices, etc) in subsequent posts, I haven’t touched on these topics yet because they haven’t been necessary in patients with COVID-19, and that is where the focus has been. But, to bring things back around, now that we are inching forward, I want to make sure I touch on all the topics I’ve been neglecting intentionally to make sure you all have what you need to effectively treat patient with COVID-19. That means we will get to postural drainage and diaphragmatic breathing, also.
So, about that force progression. That post was a long time ago, so here is the force progression I created a few years ago. My mentor and several colleagues are MDT therapists, so we were all big on force progressions. Because I saw a different kind of patient, I decided to make my own.
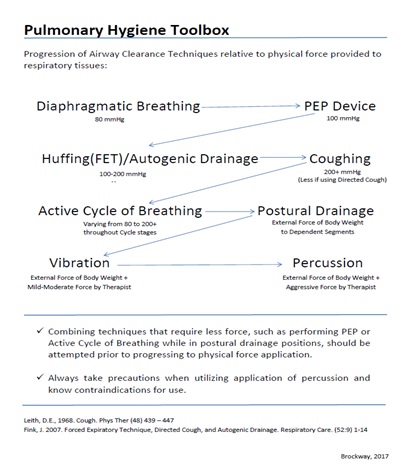
During this time of pandemic, it is important to keep in mind that, while these procedures are important for the patients who require them, they are definitely aerosol generating procedures and caution must be taken when performing them. That means wearing your your full PPE. This also means that (per the notes on the bottom of the force progression) you need to know the relative precautions and absolute contraindications for use of vibration and percussion techniques. Notice from the progression that they require the most amount of external force. If you’ve performed these procedures, you know that you can’t effectively mobilize secretions with white glove force. You’ve got to get your elbows in to it (you’ll see what I mean).
Vibration and/or percussion should also not be utilized in isolation of other interventions. These interventions need to be incorporated in to a pulmonary hygiene program that includes several other aspects of care such as postural drainage, pharmaceutical secretion management (such as with inhaled respiratory medications), and exercise-based interventions to promote the highest level of effectiveness and patient outcomes. Typically, these more forceful interventions should only be utilized for patients who have difficulty clearing large amounts of secretions, such as those with COPD or cystic fibrosis.
You can learn a whole lot more about COPD HERE, but let’s talk about why you may need to utilize this intervention. COPD is symptomatically comprised of chronic cough and hypersecretion. These symptoms are present because of bronchiectasis, or the destruction of the linings of the smaller airways. These two items are independent risk factors for reduced exercise capacity in patients with chronic bronchitis (a component of COPD), as well as being associated with increased risk of infection, hospitalization, and exacerbation. Bronchiectasis can also be present without COPD, but is a typical funding in obstructive lung conditions. Hypersecretion is where vibration and percussion work their magic. When secretions thicken (based on several factors we discuss here), they become more difficult to mobilize and an increase in force is required.
Contraindications
There are going to be some great reasons to perform this intervention, but there are also some great reasons not to. Performing percussion over the following would be contraindicated:
- Recent or Unhealed Fractures
- Active or Unhealed Thoracotomy Sites
- Unexplained Chest Wall Pain (Could be occult rib fracture)
- Areas of Atelectasis or Pneumothorax (no sound or significantly diminished sound when auscultating, typically after a trauma or surgical intervention to the chest wall – like open heart procedures)
There are also some medical considerations that may indicate percussion should not be performed on a given patient:
- Long term anticoagulation therapy/Hemophilic – this could result in diffuse bruising and pain or deeper bleeding.
- Long term use of corticosteroids as they weaken bone tissue and increase the risk of fractures, even with minimal force. This may not be an absolute contraindication depending on the degree of cortical bone loss. Weigh the risks clinically. If you have no other option and your patient is immobile… keep in mind the medical conditions that require long term use of corticosteroids.
- A patient with unstable chest pain – percussion would be very uncomfortable and increase chest pain. If chest pain is unstable angina, you have bigger things to worry about.
- Hyper-Reactive Airway Disease/Related airway conditions – this is a relative contraindication, not an absolute. These patients may be the ones who really need this type of intervention, so use with caution and use your clinical judgement. You’ll need to decrease your force and utilize less FET force also to prevent bronchospasm.
- If you suspect in any way that there may be a pulmonary embolism present – This is a much bigger concern than consolidation and needs to be addressed medically before any further intervention as it is a life-threatening condition.
Starting off…
You need to know where on your patient you are planning to do these interventions. Percussion and vibration are not to be used globally except in certain situations. Children and adults with cystic fibrosis that require long term secretion management can utilize global vibration and/or percussion by way of a HFCWO (High-Frequency Chest Wall Oscillation) machine. (Yes, adults can get cystic fibrosis. I had a lung transplant patient who was 31 and wasn’t diagnosed with cystic fibrosis until the age of 16. One of my friend’s husbands was recently diagnosed with cystic fibrosis in his 50s.) Some patients with COPD or other obstructive lung diseases may also require this extra help, but they are the exception, not the rule. So, back on point, how do you know where to apply your intervention?
You have to auscultate. Take a listen to your patient. Do it systematically and listen to where you hear the largest amount of secretions peripherally. Ronchi are a good indication of large amounts of secretions in large airways (also bad), and crackles are good indications of secretions in smaller airways. The overall goal of airway clearance is to move secretions from the periphery to the central, larger airways so they can be expelled. Listen for the peripheral crackles and perform your airway clearance interventions over those areas. THEN LISTEN AGAIN! That’s how you know if your interventions were successful and will indicate whether or not you need to move across and/or down in the force progression (above). You can also consider your intervention successful if it triggers a productive cough! That’s the whole point, isn’t it? You can read more about successful lung auscultation HERE.
Talk to your patient. Let them know what you need to do, why you need to do it, and what that will entail. Give them the power to control the interventions, in that they can stop you at any time if they become uncomfortable. Talk to them during performance (this will come up again later) so they feel comfortable communicating with you. Many patients feel like they must hold still, be quiet, and just endure interventions because a medical person is telling them to do so. Don’t be that person. Make your patient part of the intervention.
It is recommended in several articles I’ve read, however, most of them do not provide a source, to ensure you are monitoring your patient’s oxygen saturation via pulse oximeter while you are performing manual interventions for secretion mobilization. I can see the logic because if you have a large amount of secretions gather in the large airways, they could potentially block the airway. However, I’d also say that’s the point and you need to finish up your intervention with an FET to produce expectoration to remove the blockage. We will talk about that at the end.
AAANNNDDD FINALLY… Put your patient in the appropriate postural drainage position, as best as they can tolerate, prior to providing either or both of these interventions. They won’t be nearly as effective if the patient is not in the correct position, or at least, in a position that partially supports the gravity-assisted flow of the secretions.
Vibration
Vibration is a great tool to use for patients who cannot tolerate percussion, as the forces are different and less ballistic. Vibration is exactly what it sounds like. You place your hands on the patient and apply a deep vibratory force into the segment you are intending to treat. I actually find this to be more fatiguing for me than percussion. I also feel like it isn’t as effective as percussion, but that’s personal bias only.
Percussion
Percussion is different from vibration in that it requires repeated ballistic force being applied to the affected segment of the lung. This takes special positioning of the hands on the part of the clinician, as well as intentional movement to prevent fatigue. You’ll also want to regularly assess your patient’s tolerance as well as your own technique which can be done simultaneously! Check out the video to see what I mean.
Finish it up right!
Like I said above, none of these are great on their own. They need to be utilized in combination with other airway clearance techniques. FETs (short for forced expiratory techniques) are great and have a strong evidence base. Examples of FETs are, positive pressure, huffing, deep coughing, directed coughing, or the active cycle of breathing. My personal preference is to alternate percussion with FETs to improve patient tolerance to the more forceful treatments. It gives them a break in between to recover. I have no evidence for this other than anecdotal, but patients seem to appreciate the rest break. And don’t forget: LISTEN AGAIN!
Remember that percussion and vibration are utilized to mobilize secretions from small peripheral airways to the larger central airways. So you need to keep the secretions moving from that point all the way out of the airway. Follow up your manual interventions with some huffing, the active cycle of breathing, some intentional coughing, a PEP device, or just some deep breathing. These techniques will move those secretions from the larger airways to the trachea and then out.
What does the evidence say about all this?
So, for transparency, I’ll tell you that there isn’t much evidence on these interventions. You’ll find some, but not nearly as much as interventions like exercise. And much of the evidence is a bit older. It seems like the research done on these topics kind of stopped in 2010. There are a few newer ones but you have to dig pretty deep.
And as far as safety goes, even though we see a long list of absolute and relative contraindications, these are relatively safe interventions as long as you follow the proper clinical guidelines, force progression, and patient tolerance. Even in the most effected level of COPD (GOLD 3-4), invasive pulmonary oscillation and percussion is utilized safely (Those machines we talked about above). That’s mechanical force! That isn’t graded the way humans grade force. A machine will apply as much force as you tell it to regardless of patient tolerance, clinician comfort, or effectiveness. Yet, still, it has been found to be completely safe when administered by skilled professionals.
The evidence we have available, and I’ve had to go global here, tells us that manual interventions for acute exacerbations do not prevent future exacerbations. However, manual interventions for acute exacerbations do improve patient perception of dyspnea which is the number one complaint they will have. So, address their number one complaint and you may be their favorite person! Not every person who has an obstructive condition will be able to clear their secretions on their own, even with all the marvelous instruction you have provided, so you have to have manual interventions in your back pocket.
Do you perform manual interventions for airway clearance? What is your favorite combination for moving large secretions? Tell me in the comments!
More from the Pulmonary Rehab Toolbox…

Airway Clearance Techniques
SAVED THE BEST FOR LAST! COPD Management bonus content is here and it’s a special treat fo you!

Pulse Oximetry and O2 Saturation
SO MUCH BONUS CONTENT! One of my favorite posts on COPD management – Let’s go for a ride down the river…

Spilling the Box of Pearls: All the Tips on Supplemental Oxygen Management
Can’t get enough BONUS CONTENT! Still managing COPD but struggle with the oxygen? I’ve got you…
Something went wrong. Please refresh the page and/or try again.
References:
Chakravorty, I., Chahal, K., & Austin, G. (2011). A pilot study of the impact of high-frequency chest wall oscillation in chronic obstructive pulmonary disease patients with mucus hypersecretion. International journal of chronic obstructive pulmonary disease, 6, 693–699. https://doi.org/10.2147/COPD.S22896
Fink J. B. (2002). Positioning versus postural drainage. Respiratory care, 47(7), 769–777. Retrieved from https://pubmed.ncbi.nlm.nih.gov/12088547/
Fink J. B. (2007). Forced expiratory technique, directed cough, and autogenic drainage. Respiratory care, 52(9), 1210–1223. Retrieved from http://rc.rcjournal.com/content/52/9/1210/tab-pdf
McIlwaine, M., Bradley, J., Elborn, J. S., & Moran, F. (2017). Personalising airway clearance in chronic lung disease. European respiratory review : an official journal of the European Respiratory Society, 26(143), 160086. https://doi.org/10.1183/16000617.0086-2016
Nicolini, A., Grecchi, B., Ferrari-Bravo, M., & Barlascini, C. (2018). Safety and effectiveness of the high-frequency chest wall oscillation vs intrapulmonary percussive ventilation in patients with severe COPD. International journal of chronic obstructive pulmonary disease, 13, 617–625. https://doi.org/10.2147/COPD.S145440
Shen, Y., Huang, S., Kang, J., Lin, J., Lai, K., Sun, Y., Xiao, W., Yang, L., Yao, W., Cai, S., Huang, K., & Wen, F. (2018). Management of airway mucus hypersecretion in chronic airway inflammatory disease: Chinese expert consensus (English edition). International journal of chronic obstructive pulmonary disease, 13, 399–407. https://doi.org/10.2147/COPD.S144312
Torres-Sánchez, I., Cruz-Ramírez, R., Cabrera-Martos, I., Díaz-Pelegrina, A., & Valenza, M. C. (2017). Results of Physiotherapy Treatments in Exacerbations of Chronic Obstructive Pulmonary Disease: A Systematic Review. Physiotherapy Canada. Physiotherapie Canada, 69(2), 122–132. https://doi.org/10.3138/ptc.2015-78
Westerdahl, E., Osadnik, C., & Emtner, M. (2019). Airway clearance techniques for patients with acute exacerbations of chronic obstructive pulmonary disease: Physical therapy practice in Sweden. Chronic respiratory disease, 16, 1479973119855868. https://doi.org/10.1177/1479973119855868

One thought on “Vibration & Percussion”