
HFNO stands for High Flow Nasal Oxygen. This is something that was used frequently in patients who were desaturating quickly with symptoms of COVID-19. It has the ability, through the use of several different devices or setups, to deliver very high concentrations of supplemental oxygen to patients with advanced pulmonary diseases or conditions. In the physical therapy world, we don’t see these devices used very often unless we frequently work in ICU or with patients who have chronic disease, so I thought I would give you a run down of devices and what they look like so you can recognize HFNO when you see it and know what that implies for your interventions.
Improving the ventilation of oxygen will hopefully improve the amount of oxygen that gets diffused and perfused. This can be done by positioning, removing obstructions through airway clearance, bronchodilation to increase the space for more oxygen to get into the lungs, or by increasing the overall amount of supplemental oxygen. Given that bronchodilators can be contraindicated and/or have serious side effects and patients need something a bit faster than airway clearance techniques, supplemental oxygen tends to be a first line of treatment. This supplemental oxygen can come in different types:
- Compressed gas – we typically see these green canisters everywhere, but oxygen delivered from a concentrator also fits this description.
- Liquid – also called Helio, oxygen is distilled to a liquid for greater storage capacity. Hospitals typically have large storage tanks (called “dewers”) of liquid oxygen which is evaporated on site and then delivered to patient rooms on gas form. Helios can be used in the home setting, as well. The tanks look a bit different, and this is usually only used for high flow needs because compressed gas tanks run out much faster.
- Compressed gas and liquid can both be run through continuous flow or “on demand” systems.
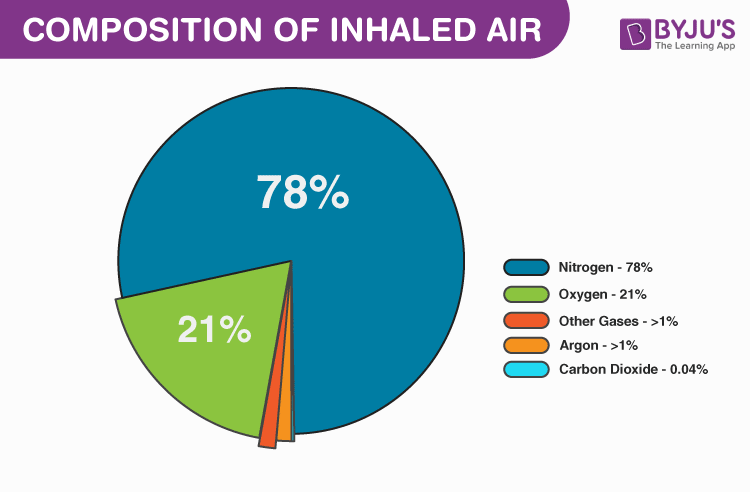
To understand high flow nasal oxygen, you need to know how much supplemental oxygen is actually being given. That depends on how many liters per minute the patient is receiving. Time to get science-y! Normal atmospheric contents break down looks like this. (See pie chart)
This matters because we have to base our supplemental oxygen calculations on “room air” which is basic inhaled air which is 21% oxygen. Every liter of supplemental oxygen added after that is roughly equal to 3% more oxygen. You can see the math is already done for you in this table.

You may be thinking, “I don’t know that I’ve ever seen anyone with 6L of oxygen… Doesn’t everyone just get 2 liters? That’s all I usually see…” Yes, 2 liters/min is a VERY common prescription for supplemental oxygen. But, as you can see form the table, that means the patient is only receiving 6% more oxygen than they would on room air (or with no supplemental oxygen). However, in the world of chronic disease, it is incredibly common to see 4 liters, 6 liters, and sometimes 10 liters.
These numbers can be fairly easily achieved with one or two concentrators as the standard concentrator goes up to 5 L/min (some go to 6, it depends on the brand). In the acutely chronically ill or, in the case of COVID-19, just the acutely ill, we sometimes see the need for much higher levels of supplemental oxygen. These levels cannot be achieved with the standard concentrator, so high flow equipment is brought in. Because this high flow is significantly irritating to the human tissues, it also must be heated and moisturized. So these devices must also provide this modification. Moisture can easily be added to a standard concentrator using a humidifier attachment, but this has to be ordered. You may have to request one of these for your patients to increase their oxygen compliance.

A few of the devices you may see…
Some of the appliances and devices you’ve probably seen can be utilized to deliver high flow oxygen if necessary. A standard reservoir mask like this one (aka partial rebreather or nonrebreather depending on the construction) can deliver high concentrations of oxygen (up to 1.0 FiO2 or about equal to 25 L/min) if the flow rate is high enough. You may have seen these in emergency departments or being used by first responders.
![Buy Oxymizer Disposable Oxygen Conserver [Oxygen Therapy]](https://cdns.webareacontrol.com/prodimages/1000-X-1000/1/r/12520205933Drive-Oxymizer-Disposable-Oxygen-Conserver-L.png)
Conserver masks can come in many different types, though, and there are some that are seen only in certain situations to deliver high flow oxygen. These masks collect oxygen in their reservoir and then feed this oxygen back to the patient at the higher collected concentration. Different types are chosen based on patient tolerance and need. These masks can be really great for patients who need to eat with their high flow oxygen because it doesn’t utilize a rebreather style mask that covers the mouth. These can also be utilized in combination with liquid oxygen (instead of with a concentrator). Liquid oxygen (sometimes called Helio) increases the amount of oxygen that can be stored in one place. Hospitals tend to have a liquid oxygen supply that is evaporated and then sent to rooms to provide oxygen to patients. These are some of the most common high flow masks I’ve worked with.

There are also some high flow devices that are a little more standard in their appearance. They look similar to a regular oxygen cannula, but they have a wider inside diameter to allow for increased flow rates.
And remember how I said that this air needs to be heated and humidified so that it’s actually tolerable? Here is the device that provides that! This is the Venturi. This bad boy can deliver anywhere from 20-60 L/min of supplemental oxygen! This oxygen at such a high flow is used to wash out dead air space like with people who have advanced COPD. This also creates a bit of PEEP to improve ventilation, like a CPAP. This is another one of those things that I wish I could have in my trunk!
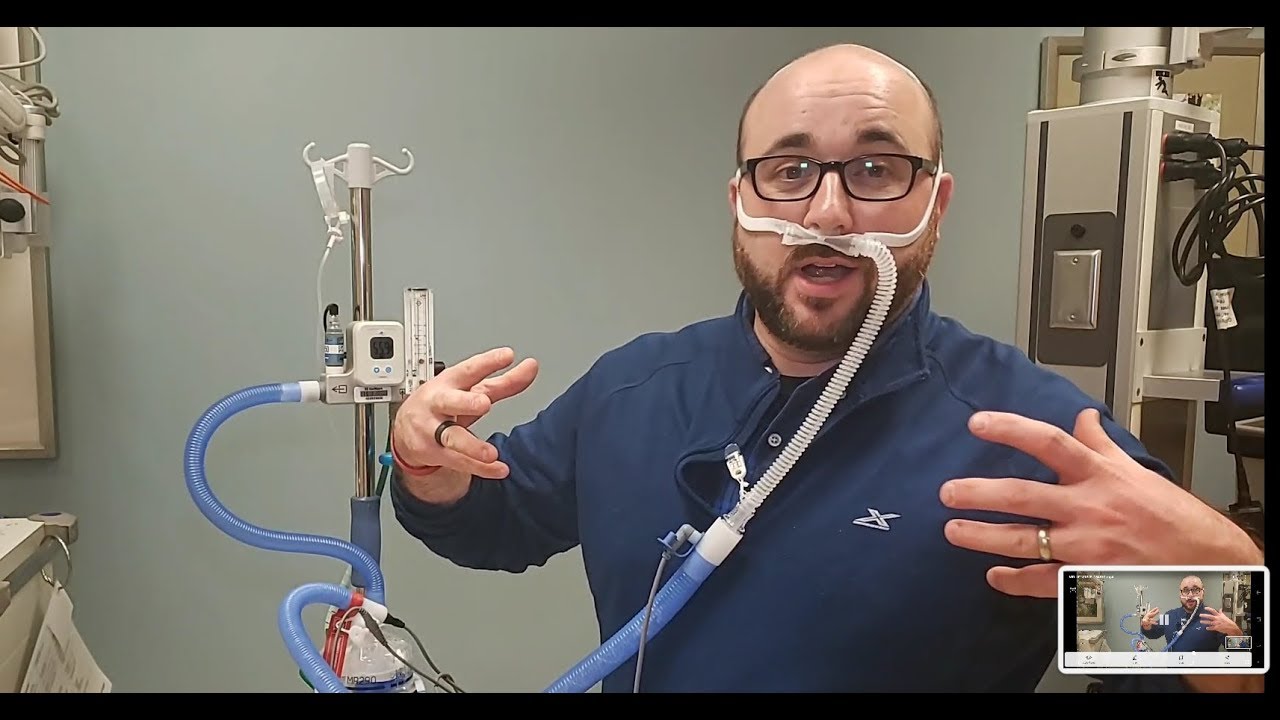
This heated humid air actually helps the anatomical function of your soft tissues so they can diffuse oxygen better. Without the heat and humidity, large amounts of mucous would develop and actually block airways. This specific device actually allows clinicians to adjust the FiO2 to help prevent oxygen poisoning for those who rely on hypoxic drive. This type of device can also be helpful for your patient on BiPAP who needs to maintain saturation while eating as it utilizes a nasal delivery, so the mouth is not obstructed while the airways remain patent.
So, what does all of that mean for your therapy? Well, if a patient is on high flow oxygen and you aren’t seeing them in the hospital, odds are they have a pretty advanced stage respiratory disease. This can be COPD, cystic fibrosis, pulmonary fibrosis, or any other condition that results in chronic hypoxia. Many of these mask types are portable (with the exception of the last one pictured), but the portable oxygen supply may be short. High flow means they will run out faster. It also means that portable concentrators are probably not an option as most of them are limited at 4 L/min. High flow stationary concentrators are available that go up to 10 L/min, but your clinic would need to have one for the patient to use as they are not portable. Ultimately, this patient either needs to be connected to a wall-mounted oxygen source with a reservoir/conserver mask (this can be done in physician offices, typically), or they need to be seen at home.
If you are seeing them at home or in a sub-acute facility, this means you need to be sure of a couple things:
- You are monitoring oxygen via pulse oximetry with everything, including rest
- You are auscultating their lungs at every visit to assess function and/or change in presentation (pneumonia starts quickly when there is a lot of dead space or secretions)
- You are taking a full set of vitals at least once during the visit
- You are ensuring titration orders are in place and correct
- The patient has a back up supply of oxygen somewhere that can last up to 24 hours in case of power outage (Kilo tanks or Helio)
- You have educated your patient on frequency of cleaning and discarding oxygen equipment to prevent respiratory infections
- You are still exercising them to an appropriate intensity (60-80% HRmax) for as long as they can tolerate
Yes, I promise, you can still exercise patients who have to utilize HFNO, even up to 85% HRmax. I’ve had patients running 16 L/min alternating squats for strength and amplitude exercises to improve their rib and spine mobility. They will get to their target heart rates pretty quickly and need their activity attenuated to maintain that level without quickly exceeding it.

Yea, that’s me doing those exercises. See that nonrebreather reservoir mask? She called it the “bag mask”. See that string hanging from my pocket? That’s my pulse oximeter. As always, she was using her 16 L/min to laugh at me.
Do you see patients who use HFNO? What are the most common diagnoses? Tell me in the comments!
More form the Pulmonary Rehab Toolbox…

Airway Clearance Techniques
SAVED THE BEST FOR LAST! COPD Management bonus content is here and it’s a special treat fo you!

Pulse Oximetry and O2 Saturation
SO MUCH BONUS CONTENT! One of my favorite posts on COPD management – Let’s go for a ride down the river…

Spilling the Box of Pearls: All the Tips on Supplemental Oxygen Management
Can’t get enough BONUS CONTENT! Still managing COPD but struggle with the oxygen? I’ve got you…
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!
References
College of Respiratory Therapists of Ontario. (2013). Oxygen therapy clinical best practice guidelines. Retrieved from http://www.crto.on.ca/pdf/PPG/Oxygen_Therapy_CBPG.pdf.
Tepper, S., Wruble, E., Stewart, E. (2020). Anatomy, histophysiology, and pathophysiology of COVID-19. Pacer Project. Retrieved from https://YouTube.be/w7bafww8IWo

Follow @DoctorBthePT on Twitter for regular updates!

9 thoughts on “HFNO”