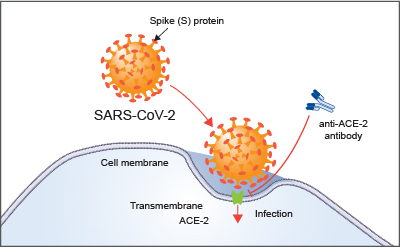
We can basically thank our old friend sepsis for the presentation of strokes in patients with COVID-19. This virus has changed so much and so frequently since it landed stateside, but there was evidence from its China days that neurological involvement was implicated. Initially, though, it all started in the lungs. We talked about this a lot over the last several posts, but ACE2 receptors, the primary receptors that have an affinity for the SARS-CoV2-19 virus, are present in the endothelium of the heart, arteries, kidneys, and in the glial cells in the brain. This is not new. I didn’t look very hard and found articles from 2005 that indicated that we’ve known this for a while. (Corona viruses are also not new, they just only really impacted animals prior to the SARS-CoV-1 and -2 outbreaks, so we’ve been researching this for a while.) Some evidence exists that suggests ACE2 receptors being present increase the risk of end-organ damage to that specific tissue because it receives the virus more easily. So here are some mechanisms by which COVID-19 can result in cerebrovascular accidents of different varieties.
Just a warning, we are going to get REAL SCIENCEY here!!! I love to tell my students to go back to the basics of what they know. Our basic physiology and anatomy knowledge is really important here. It’s important pretty much everywhere, but especially when discussing disease mechanisms. I know this stuff is tough but I’ve tried to make it straight forward. The better we understand our enemy, the more equipped we are to go in to battle.
Angiotensin converting enzyme 2 (ACE2) is on the outer surface of lung tissue which is why the lungs have been most heavily affected by COVID-19. We know the virus invades the lungs, overwhelms the natural protective factors due to expedited viral replication, destroys the lung parenchyma, and causes interstitial fluid build-up. Damage of the basement membranes of the alveolar pneumocytes results in scarring because the pneumocytes cannot restore themselves to their original location or function without the guide of the basement membrane.
MECHANISM 1. So what happens with ACE2 receptors in the heart? ACE2 receptors in the heart function to lower blood pressure via changes to stroke volume when they are activated. When these receptors are impaired or destroyed due to infection with the SARS-CoV-2 virus, blood pressure begins to elevate under little control. The more receptors damaged, the more blood pressure elevates. We know that when a hypertensive state is sustained or just very severe, a cerebrovascular accident of either ischemic or hemorrhagic etiology is possible. Then you pair this with ACE2’s function in the vasculature (vasoconstriction) and pressure increases even higher. If the patient has an underlying comorbidity (like A-Fib) that could result in clotting, ischemic etiology would be more likely as this pressure would dislodge a clot. If not, a hemorrhagic event could be suspected.
MECHANISM 2. How about the brain? ACE2 receptors are on glial cells but the blood-brain barrier is supposed to give us an extra level of protection against these types of infections. Unfortunately, the SARS-CoV-2 virus attacks the endothelium of capillaries and destroys this single-cell barrier (the blood-brain barrier) allowing the invasion of SARS-CoV-2 virus in to the neuroglia. These types of infections tend to result in cerebrovascular accidents of the hemorrhagic etiology. This can also result in peripheral nerve injuries to a lesser extent. It is suspected that this is also why people have chemosensory changes, confusion, and delirium as symptoms of COVID-19 before treatment.

MECHANISM 3. We know a patient with COVID-19 demonstrates increased blood viscosity, decreased perfusion, general ischemia/hypoxia, and requires increased cerebral blood flow to maintain function (because this blood is poorly oxygenated). As PaCO2 and PaO2 become altered, and the patient becomes hypercapneic, cerebral autoregulation which regulates intracranial pressure (ICP), is impaired. This state of increased pressure can also result in a hemorrhagic accident. Unfortunately vasopressors do not cross the blood-brain barrier so we cannot modify this via this mechanism and perfusion remains poor.
MECHANISM 4. COVID-19 viral RNA may attach to capillary endothelium when blood born (hello, again, Mr. Sepsis). We know this can result in a cytokine storm with end-organ damage targeting pretty much any system you can name. Included in this list of systems is the clotting cascade and endothelium themselves. This results in thrombosis and platelet activation which overall produces clotting. It is known that patients with COVID-19 develop pulmonary embolisms at an increased rate. This could be one of the reasons (along with immobilization, medications, etc). These clots can also go pretty much anywhere, including the heart, brain, kidneys, etc… More than 70% of people who perished due to COVID-19 demonstrated intramuscular thrombosis! This is NOT normal. So all these organs systems continue to be at risk for serious injury due to VTE risk. This risk continues after the ICU and rehab phases of this condition and persists with the patient. We don’t know how long yet. The risk of ischemic CVA increases with respiratory infection even in non-COVID-19 patients.
Here’s the really tough part. Some of the things we have to do to sustain life in a patient with COVID-19 may actually be causing cerebrovascular accidents or other neurological complications and extending the timeline of recovery. However, the risk/benefit analysis is pretty grim: definitely die now or maybe not die later. Our physicians and patients have really tough choices to make.
MECHANISM 5. A very high PEEP is required for mechanically ventilated patients with COVID-19, higher than most other diagnoses require. Positive End-Expiratory Pressure (PEEP), not to be confused with PEP, is pressure applied at the end of exhalation to maintain the patent airway. PEEP is typically seen in those who use CPAPs or BiPAPs. This must be more than the atmospheric pressure and more than the passive pressure of exhalation. Many articles I’ve seen talk about 5 cmH2O as a standard starting point for most patients. Patients with COVID-19 are requiring 30+ cmH2O to maintain their airways (I’ve read cases of 60+ cmH2O reported). The use of higher PEEPs results in increased ICP which can result (as we have already mentioned) in neurological complications and stroke.

MECHANISM 6. Proning itself does not cause neurological complications, but it is difficult to maintain in most patients without the use of sedatives. If you think about the position with a giant tube through your trachea, lines and leads coming off every inch of you, and a generally uncomfortable hospital bed, you’d probably want sedatives, too. Sedatives can also be helpful for managing the discomfort that comes with sepsis. However, they can decrease cerebral perfusion and metabolism which further decreases cerebral autoregulation. If the patient is proned and positioned in a way that compromises the jugular vein, ICP can further be increased and we end up with similar issues as in mechanism 5.
Thankfully, ya’ll, I see a lot of room in here for rehab clinicians to intervene.
- TAKE VITALS – every patient every time, more than once, at rest and with activity, as often as is clinically indicated, and then maybe a few more! Monitoring blood pressure is going to be so important as hypertension is our biggest enemy here! Respiratory rates at rest and with activity, when combined with oxygen saturations can help determine presence of PE or DVT. Welcome to my soapbox.
- NEUROLOGICAL BASELINE ASSESSMENT – If you don’t remember what they looked like when they started with you, you have no basis for comparison if something changes! How confused were they? How delirious were they? Were they having headaches?
- POSITION SMART – Prone smart. Position well. Change positions frequently. Create a turning schedule. Take charge of positioning schedules to ensure they are maintained. Changing patient positions helps reduce PE and DVT risk. Prevent peripheral nerve injuries and ICP elevation.
- MONITOR DRUG USAGE – Ensure patients are taking their medications as prescribed. Review their medications for changes or questions. Make sure they can access their medications and can get their refills when needed. Managing a patient’s medical comorbidities, like A-Fib, well reduces the risk of complications like neurological insult.
- ADVOCATE – in the ICU for early mobility and breaking or reducing sedation as early and as often as possible while maintaining a hemodynamically stable patient in conjunction with your interdisciplinary team. Reduce the risk of DVTs and PEs, reduce the effects of sedatives, and reduce the overall cognitive impact.
You guys are working miracles out there! Tell me how you and your team are addressing the risks of CVA for COVID-19 in the comments!

Pressure… Pushing Down On Me…
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…

Dehydration
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease

Chronic Disease Part 3: Urinary Incontinence – Part 1
NEXT FEATURE IN THE CHRONIC DISEASE MANAGEMENT SERIES!!!
Let’s learn how to manage incontinence! But wait, that’s not a chronic disease, is it? Well, let’s take a look and find out!
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!

Follow @DoctorBthePT on Twitter for regular updates!
References
Levenhagen, K., Gorman, S., Verma, A., Kumble, S., Lopker, M. (2020). Physical Therapy Considerations of Neurologic Presentations in COVID-19. [Webinar] Viewed May 8, 2020. https://register.gotowebinar.com/recording/8523389256235766031

12 thoughts on “So Now COVID-19 Results in Strokes (and other neat things about ACE2 receptors)”