
All that work on intra-abdominal pressure really kept taking me down the road of incontinence management, but that post was already long enough, so this one is going to get it’s own feature. I work with patients on managing urinary incontinence in every setting, so let me take you through some basics of how to do this. I am not a certified pelvic floor Physical Therapist and I only claim to know the absolute basics, but for many people, the basics are pretty helpful, and can at least buy time until they can get to a specialist if they need to. You may be thinking, “Why is this person who does mostly cardiopulmonary all day want to talk about urinary incontinence?” Well, most of my patients who have cardiopulmonary conditions like COPD or Heart Failure either have secondary effects of those conditions that cause incontinence or take medications that cause incontinence. So, out of necessity, I had to learn how to address these things.
This is a huge topic, also, so it’s going to be broken in to two parts. The first part is heavy on the what and the why so that you can have a really good understanding of the importance of managing this condition in patients across different setting. This will also help you have some great ideas for how to document what you are doing and why.
Why Is Urinary Incontinence Such a Problem?
Urinary incontinence straight up leads to disability. It may not be immediate, or it may be, but it’s a slippery slope and a short road. Urinary incontinence is extremely common, but it is NOT normal. It happens to both men and women, but definitely more often in women. When I was in PT school, we learned that about 80% of women will experience incontinence of some kind at some point in their life. Further research showed that this is also true of about 54% of men. That’s because incontinence doesn’t just come from childbirth, believe it or not. You can read more about things that cause stress incontinence in the post about intra-abdominal pressure, but we will go in to some detail here.
Urinary incontinence is the #1 reason women are placed in a facility as they age. That is because it becomes pretty hard to manage. There are many products that require purchasing, so it also becomes expensive. Incontinence is also among the leading causes for institutionalization of men as they age. This facility placement also typically leads to these men and women becoming dependent in their toileting, because they transition from what was otherwise a stress, urge, or mixed incontinence, to a functional incontinence. You can read more about that below, but basically, if there is no one available to help you, you eventually get to a point where you just go. This has been shown to increase depressive symptoms and severely impact overall well-being. Urinary management was the most-often reported impaired ADL in people over 65 years old, but it happens at ANY age.
And, finally, it is all potentially preventable. All of the journals cited in this article and several geriatric organizations agree that promoting continence or management of continence in the geriatric population is the most important factor in maintaining independence and well-being. But, it’s not just about the geriatric population, right? I did plenty of treatment for incontinence in outpatient orthopedics for patients of all ages, both men and women. Unfortunately, we often don’t see younger patients in therapy specifically for incontinence, but they do tend to come in for other issues… specifically back pain, hip pain, and core weakness! The incidence of stress urinary incontinence coexisting with low back pain is high, especially in women. This is where you come in. Let’s learn a bit more about Urinary Incontinence.
Types of Urinary Incontinence
Stress. We talked A TON about this stress in the article on intra-abdominal pressure regulation, so you can the details there, but overall, if you place enough stress on the bladder, it will empty. This type of incontinence happens when you cough, sneeze, stand up, hold your breath, turn over, strain… pretty much anything that can increase intra-abdominal pressure. This type is more common in women than in men, but, if you’ve seen men with abdominal hernias, you know it exists in men, too.
Urge. Sometimes called “key-in-door” incontinence, this type comes from a sudden and unexpected urge to urinate. This urge may be neurologic or reflexive in nature, like you always have to go when you get home from work so when you get to the door, you have the feeling that you have to go. It has been shown to be due to the combination of some type of reflexive or neurogenic trigger AND an overactive detrusor muscle (the muscle that surrounds the bladder). This urge can sometimes come from bladder irritation, too, and we will talk about what that means later. This type is actually more common in men than in women.
Mixed. This is the descriptor for some type of combination effect of both stress and urge incontinence.
Overflow. This one is pretty self-explanatory. When your bladder gets too full, it HAS to empty, whether you are ready or not. Sometimes, you just wait too long. Or, as with otherwise potty-trained children, they can get distracted by playing, and then they just go. Overflow incontinence can also happen when bladder emptying is impaired. This can happen by many mechanisms such as prostate enlargement, scarring of the urethra, detrusor weakness, or a bladder prolapse (cystocele). If the exit is blocked, nothing comes out.
Functional. This is the worst type of incontinence because it is 100% preventable. Functional incontinence is incontinence that happens when you can’t get to a bathroom safely or don’t have the help to manage the bathroom tasks that you need to perform. It can also result from shame, embarrassment, weakness, balance impairments, homelessness, and environmental barriers. Here is a clip of me talking about functional incontinence so you can get an idea of how this happens:
Doctor B talking about functional incontinence in the aging population Neurogenic. Neurogenic bladder results from some type of neurologic disruption to the bladder and its systems. This could be in a patient with spinal cord injury who cannot feel that their bladder is full. They no longer have the connections to the reflex mechanisms that send their brain that signal, so they have to perform intermittent catheterizations to empty on a regular schedule. Other neurological conditions, like Multiple Sclerosis, Cerebrovascular Accidents, Parkinson’s Disease, and many others can impact these reflex loops or their centers in the brain and result in a neurogenic bladder. Trauma can also lead to this condition if there is damage to the sympathetic (T10-L2) or parasympathetic (S2-4) trunks that innervate the detrusor muscle.
And, as with many things, the likelihood of urinary incontinence increases with age. This is due to many factors, but the compounding of these factors, like the increased number of comobordities accumulated with age, increases the risk of urinary incontinence. There are several health conditions that result in different types of urinary incontinence by direct of indirect mechanisms. The American Society of Nephrology produced this great table that gives you a good overview of the things that can cause urinary incontinence.
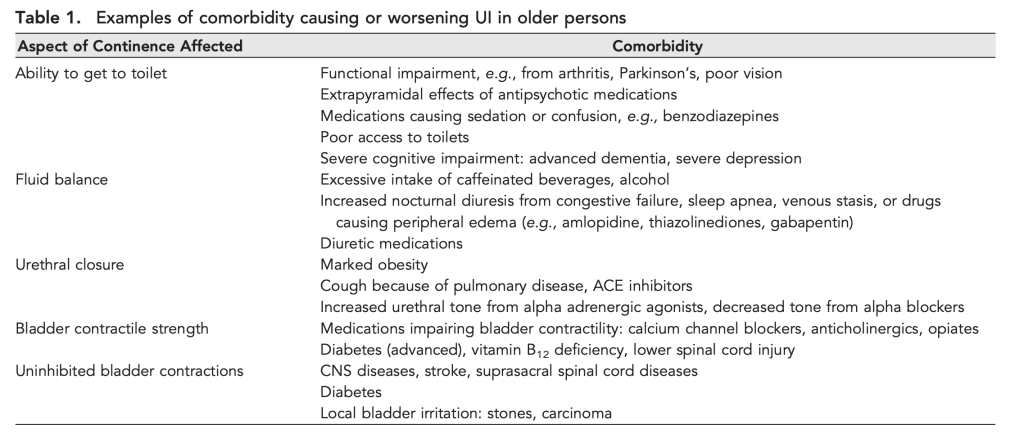
I want to point out, specifically, the line in this table on “Bladder contractile strength”. There are so many things that change the ability of the bladder to contract appropriately, and most of my patients have at least one of the items on that list in their medications list of past medical history. The bladder is surrounded by a muscle, right? And it has neurological inputs and outputs and can be strengthened, just like any other muscle! And you are a Physical Therapist, isn’t that what you do? So let’s take the first step:
Identifying Urinary Incontinence
No one really wants to talk about it. No one really wants to admit it. So, you can’t just ask, “Do you pee your pants sometimes?” because it won’t get you any useful information. In the home setting, it’s probably most beneficial to just look around. You’ll see what you need to see if someone has incontinence. There will be products readily available in the bathroom, and there may even be soiled clothing laying about. In the outpatient setting, it’s a bit tougher because you can’t take as many nonverbal clues. You have to get crafy in your questions! Here’s how I go about this:

“Do you ever have any urine leakage?”
“Do you ever have any other type of leakage?”
“What about when you cough or sneeze sometimes?”
“Do you ever need to use any products for leakage like pads or undergarments?”
“How often do you need to change those in a day?”
“Do you notice you have leakage with any certain activities?”
And just because they answer “No.” to the first one, doesn’t mean I don’t ask the others. Often times I will get “No,” as the first answer, but then yes to several of the other questions. It is also incredibly important to follow up this series of questions with a conversation about how, although this is common, it is NOT normal, and can be improved or resolved very easily, even if it has been happening for a long time. You may also need to add a conversation about how pads and undergarments are only a band aid, not a solution, but we will get more into that later.
How is Urinary Incontinence Treated?
Well… here’s the thing. Most people who have it don’t treat it. They simply think it’s normal. Most of them are women who have had children and they just think that’s how things are. BUT IT’S NOT TRUE. Other treatments tend to focus on type and cause. Normalize the situation, but also normalize treatment. Many people will be ashamed or embarrassed and they will need you to coach them through that in order to make progress toward a solution.
Using liners, pads, or briefs allows urine and other body waste to stay in contact with the urethra, resulting in some of it working it’s way back in. The result, especially in older adults and those who are immunocompromised, is a urinary tract infection. Urinary tract infections (UTIs) are incredibly common (but also NOT normal) and the incidence is rising. This is a much bigger problem than most people realize and here’s why: Antimicrobial resistance, also known as super bugs. The number of hospitalizations for UTIs is rising year after year, especially over the summer months, and doctors think that this is due to patients being previously treated for UTIs but returning due to a developed resistance to antibiotics.
Urinary tract infections are hugely problematic. They are incredibly dangerous and can result in sepsis, falls, temporary or permanent mental status changes, and continually decreasing urinary health and function. All of which results in decreased functional ability, hospitalization, institutionalization, or even death. They also contribute to the aforementioned building concern for drug-resistant microbes. I may not be a pelvic floor therapist, but I’m pretty darn vocal about this! Here are the types of urinary incontinence and how they are typically treated at the present. Hopefully we can make some serious changes!
Stress incontinence. As a secondary effect of other comorbidities, stress incontinence can be treated with medications and other interventions for the comorbidities, along with retraining of how they regulate their intra-abdominal pressure. As a primary diagnosis, regulation of intra-abdominal pressure and pelvic floor strengthening exercises are usually the keys to success.
Overflow incontinence.
Treated by removing whatever blockage is present to the urethra. This typically involves surgical repair for prolapses, bladder suspension, or prostate removal. Unfortunately, these procedures come with a laundry lists of side effects and effectiveness is questioned. If the blockage cannot be removed, intermittent catheterization or indwelling catheters can be used, but have serious potential for problems.
Urge incontinence. May be due only in part to an overactive detrusor muscle, but is typically only treated using medications that target relaxation of the detrusor muscle. Unfortunately, this can result in over-relaxation of all the muscles or just the detrusor muscle which then results in several other issues. And, this treatment only treats half the problem! We now that there is a neurological component to urge incontinence.
No Treatment. Most commonly, there are those who don’t treat it, but attempt to manage it using liners, pads, or briefs, effectively allowing it to happen, but not letting anyone else know it is happening. In men, catheterizing is a common technique to address incontinence. Here’s the problem with all of that:
Infection.
This is Serious! I Need to Treat This! What Do I Need to Do?
Physical Therapists play a very large role in managing urinary incontinence. If you read through that table from the American Academy of Nephrology, I’m sure you noticed that most things on the list are things we can address in some way, whether it is a medication reconciliation, a lifestyle change, and environmental change, or physical intervention. There are going to be LOTS of options for you to chose from for your patients. There is something for everyone! So make sure to check back!
Reduce modifiable factors
Some things you can change, some things you can’t. So work with what you can change. You can’t change someone’s age, gender, or disease. You can change their location (maybe), their available help (maybe), their medications (maybe), their mental state and function (maybe), their BMI (maybe), their safety, their functional ability, their strength, their diet, and their environment. A lot of maybes… But this gives you many different avenues from which you can launch your treatment. Let’s attack the maybes first:
If you band together with some of your healthcare team, you can address some of these maybes pretty well. You can work with a social worker to get in-home help or find suitable supportive placement. I know that institutionalization is not the best answer, but sometimes it’s the only answer, and sometimes its better than being alone and unsafe, but you can also consider short term rehab facility placement. You can work with the primary care doctor (or urologist and cardiologist, if you are lucky) to change medications or reduce dosages to reduce cognitive effects, stabilize fluid dynamics, and reduce fall risk. You can work with family to arrange for in-home assistance. And, as a skilled rehab provider, you can get someone going on an exercise program to begin chipping away at their BMI.
Other than the maybes, we have some pretty tangible stuff in this list that Physical Therapists are pretty poised to address. These are some of the things I was talking about when I mentioned the lifestyle changes. Let’s take a look at those:
01
Environment
Take a look around. Reduce barriers, ensure safety. Turn lights on, make paths short and straight. Make sure they have the appropriate assistive device.
02
Functional Ability
The path is great, but we have to get to it. Make sure they can get out of a chair by elevating it if needed.
03
Diet & Fluids
More water is better. I know this is counterintuitive, but it’s important. Reduce or eliminate bladder irritants.
04
Strength
Lower extremity strength, Upper extremity strength, core strength, pelvic floor muscle strength… Pick one or several, depending on your patient’s needs.
Bladder Irritants? Yes, that’s a thing.
Over-concentrated urine is a bladder irritant, so cutting water intake should not be an option. Keeping a patient with heart failure or ESRD within their approved water intake is important, but reducing it is not a solution. Many patients like to cut out liquids before bed so they won’t have to get up to use the bathroom at night. Although this strategy sounds plausible, it results in increased urine concentration and your patient will actually have to get up more often. Patients who are returning to a healthy water intake after restrictions will initially experience an increase in urinary frequency, but their body will regulate with time. If your patient doesn’t like water, have them gently flavor it with flavor drops (not powder or sugar-based drink flavors) or fruit.
Some food and drinks are also bladder irritants. As much as it pains me to say it: Coffee. Technically, caffeine is the culprit, though. Let me tell you this little pearl: DO NOT tell your patient to stop drinking coffee. You’ll lose them immediately. Ask them, instead, to alternate a cup of coffee with a cup of water. Other highly caffeinated drinks like soda are also on this list, as well as highly acidic foods and liquids. Citrus fruits, tomato products, and spicy foods will all result in increased urge or frequency or both. However, diluting these irritants can help, so keep the water flowing.
Another one that will get you gaffs if you suggest it’s removal is alcohol. Alcohol, much like coffee, dehydrates you, increases urine concentration and causes bladder irritation. Like I said with coffee, don’t suggest eliminating it, suggest diluting it by alternating with water. If your patient is treating their urinary incontinence with medications, you’ll want to advise removing alcohol completely as it has severe interactions with some of these medications.


Bladder Retraining Programs
This is where a referral to our magical friends in the pelvic floor rehab arena are called upon. We create voiding schedules for our patients with spinal cord injury, and this process is similar. If you have established a reflexive (literally, neurological reflex loop) habit of going to the bathroom at a given time of day or before/after a certain activity, your brain will learn this pattern and make it happen. These schedules can be helpful to maintain continence, but they can also be detrimental if they are not created intentionally. Remember that “key-in-door” incontinence we talked about? What if you can’t find your keys? Problem! Try going before you leave work. Then you’ll know you don’t actually have to go and you can calm your jets.
It is extremely important to remember that our body has an alarm system for a reason. Our bladder sends signals to our brain to say, “Hi there, I’m full! Time to empty me. Better find a bathroom soon.” If we don’t respond to these signals, they will intensify, “Hey, I’m telling you I gotta go, so let’s go! Now!” And as long as you get there, that’s great. The system worked. But this can go awry in two ways.
- What if you can’t get there?
This is where functional incontinence happens. If you can’t get there even though you know you have to go, you need to identify the reason. Strength, environment, endurance, etc… See the list above. If you don’t get there, overflow happens and you go anyway. - You keep ignoring the signals.
This actually creates a negative learning loop. If you ignore the signals enough, the body and brain figure out that the signals aren’t working and the bladder stops sending them. BAD PLAN. Now how the heck are you going to know when you have to go? And we end up in overflow again with no warning.
Your local pelvic floor therapist is going to be the best one to help you figure out these schedules, reflexes, and learning loops to best set up a schedule that fits your patient’s personal needs. Don’t forget that incontinence happens at all ages, so we may need to consider school and work schedules when timing bathroom breaks.
Finally… Pelvic Floor Muscle Strengthening and other Bladder Management Techniques
This is where I’m going to leave you in a bit of suspense! This post is already getting pretty long and complex, so I’m going to make treatment options an entirely different post. Stay tuned! I’ll link Part 2 once it is published.
So much to think about and so many people we can help! I once was able to resolve functional incontinence in a patient simply by having her turn on the bathroom light prior to entering. It can be that simple! Do you have a story about a lifestyle change that significantly improved incontinence? Tell me your story in the comments!
Follow my blog for more!
More on How Physical Therapists Manage Chronic Disease!

Dehydration
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease

Chronic Disease Part 4: Type 2 Diabetes – Part 2
IT’S HERE!!! The NEW BLOG POST! The next installment in the Chronic Disease Management Series on Diabetic Care is here! Let’s talk about feet!

Treating Long-COVID: Part 2
NEW POST COMING MONDAY! But I can’t give you Part 1 of Treating Long COVID without giving you Part 2! #covid #physicaltherapy #chronicdisease
Something went wrong. Please refresh the page and/or try again.
References
Ayeleke, R. O., Hay-Smith, E. J., & Omar, M. I. (2015). Pelvic floor muscle training added to another active treatment versus the same active treatment alone for urinary incontinence in women. The Cochrane database of systematic reviews, 2015(11), CD010551. https://doi.org/10.1002/14651858.CD010551.pub3
Bush, H. M., Pagorek, S., Kuperstein, J., Guo, J., Ballert, K. N., & Crofford, L. J. (2013). The Association of Chronic Back Pain and Stress Urinary Incontinence: A Cross-Sectional Study. Journal of women’s health physical therapy, 37(1), 11–18. https://doi.org/10.1097/JWH.0b013e31828c1ab3
Carvalho, N., Fustinoni, S., Abolhassani, N. et al. Impact of urine and mixed incontinence on long-term care preference: a vignette-survey study of community-dwelling older adults. BMC Geriatr 20, 69 (2020). https://doi.org/10.1186/s12877-020-1439-x
Kuchel, G. A. and DuBeau, C. E. (2009). Urinary Incontinence in the Elderly in Geriatric Nephrology. American Society of Nephrology. Retrieved from https://www.asn-online.org/education/distancelearning/curricula/geriatrics/Chapter30.pdf
Mayo Clinic. (2020). Bladder Control: Lifestyle strategies ease problems. Retrieved from https://www.mayoclinic.org/diseases-conditions/urinary-incontinence/in-depth/bladder-control-problem/art-20046597
Nuotio M, Tammela TL, Luukkaala T, Jylhä M. Predictors of institutionalization in an older population during a 13-year period: the effect of urge incontinence. J Gerontol A Biol Sci Med Sci. 2003 Aug;58(8):756-62. doi: 10.1093/gerona/58.8.m756. PMID: 12902536.
Simmering, J. E., Tang, F., Cavanaugh, J. E., Polgreen, L. A., & Polgreen, P. M. (2017). The Increase in Hospitalizations for Urinary Tract Infections and the Associated Costs in the United States, 1998-2011. Open forum infectious diseases, 4(1), ofw281. https://doi.org/10.1093/ofid/ofw281
Welk B, Baverstock R. Is there a link between back pain and urinary symptoms? Neurourol Urodyn. 2020 Feb;39(2):523-532. doi: 10.1002/nau.24269. Epub 2020 Jan 3. PMID: 31899561.
Zilberberg MD, Shorr AF. Secular trends in gram-negative resistance among urinary tract infection hospitalizations in the United States, 2000–2009. Infect Control Hosp Epidemiol 2013; 34: 940–6.

Follow @DoctorBthePT on Twitter for regular updates!
