
Make sure to check out Part 1 of this series HERE!
Let’s Jump Right In
And… moving on! I made some promises in the last post about the diabetic foot, diabetic ketoacidosis, insulin sliding scales and other medications, and using exercise to treat diabetes, so we are going to go through a few posts to cover those topics and get you ready to fully manage folks who have Type 2. This part of the series will focus on diabetic foot management.
As PTs, we frequently look at, touch, and work with people’s feet. Most people have feet and our feet are the base of our body. There is an older book out there called When the Foot Hits the Ground, Everything Changes and it was a standby resource at one of my old clinics. Needless to say, the feet are pretty important. But some populations, the diabetic population, in particular, have a pretty high risk of losing their feet (or parts of them). Amputees are a large part of my caseload and I can say that with certainty across any setting. Home health, skilled nursing, subacute rehab, inpatient rehab, acute care, outpatient… yep, lots of missing parts. Not all of them are due to diabetes, but in the Geriatric population, many are. And those are my people.
So, let’s talk about feet!

The Diabetic Foot
Because the feet are at the bottom of the body, they are typically the furthest from the heart (or the pump) and, therefore, receive blood with the assistance of gravity (because gravity helps the blood go downward). As blood vessels get further from the heart, they also tend to get smaller, and if you do some basic math, that means that the blood in your feet will likely be under higher pressure than the blood in your arms, but the difference shouldn’t be too far off in a well-functioning system. You can read more about that here.
Now, those smaller blood vessels have a lot of work to do, supplying all the small muscles, nerves, bones, and other tissues in the feet, and then return all the waste products from those tissues back to the removals systems in our body. Getting blood down to them is not usually an issue, but because blood has to work against gravity to return to the source (the heart), our body has valves in the veins to help keep the blood from flowing back down to the feet after it has left. This process is also assisted by muscles in the legs that squeeze the arteries and veins as they contract and relax. If you’ve ever been told about ankle pumps or have taught someone to do ankle pumps, this was probably the reason behind that activity: help pump blood, waste, and fluid out of the feet and against gravity.
So far, this should all sound pretty basic, which is great! because most of these things to this point aren’t that complicated. However, when you add diabetes to the mix, things start to change and the whole system begins to become far more complicated. Let’s talk about peripheral vascular disease for a minute.

Now, I could talk about vascular disease pretty much all day, but the gist of it is that when blood glucose (or “blood sugar”) levels go unchecked, this causes damage to the endothelium (the most intimate and fragile layer of the blood vessels). This damage results in scar tissue and other things that shouldn’t be there getting deposited within the wall of the blood vessel. This scarring and buildup cause the blood vessel walls to harden and, eventually, the muscles within the walls of the arteries do not work anymore. The artery just becomes a stiff pipe that cannot respond to increased or decreased demand for blood and oxygen from the tissue below (in the foot). The tissues of the foot are then starved for these vital substances and cannot maintain good tissue health. And now we’ve gotten to where we are going… It’s a bit of a long road and it takes some winding turns, but let’s talk about what all that means. We will go by tissue type:
Nerves
Nerves require a blood supply to function. Nerves are also myelinated (or covered in fat) which helps them carry signals faster than they otherwise could. This fat also requires blood supply. When nerves don’t get the oxygen and nutrients they need, they can’t send signals properly or quickly, which can result in erroneous signals or a lack of signals. In patients with diabetes, we often hear this called neuropathy. And, in people with diabetes, this neuropathy happens distal (or furthest away) to proximal (closest) resulting in a stocking-style presentation of paresthesias or anesthesia.
Of note, in the upper extremities, it can present in a glove-live pattern. I see this more often in people who have Type 1 diabetes, but we are talking about the feet here.
If the nerves aren’t sending signals properly, or at all, the foot can’t feel the sock or shoe it is in. This can result in pressure sores from improperly fitting shoes or broken-down shoes. Wounds can get infected pretty easily when they are on the feet, so sepsis ensues and this is how feet are lost. The foot also can’t feel the ground, and this is a big one because that implies effects all the way up to the brain. Here’s what I mean: If the foot can’t feel the ground, then the brain has to use other mechanisms to ensure it is on the ground, like the vestibular and visual systems. These three normally all work together, but now only two are working properly, so that patient has lost one-third of their balance systems. Now we have an increased risk of falls.

Just as there are blood vessels to nerves, there are also nerves to blood vessels, so their function is intricately intertwined. There are intimate interactions between the nervous and vascular systems, and malfunctions in one will result in malfunctions in the other. This also contributes to neuropathy and several other neurovascular issues throughout the sympathetic and parasympathetic nervous systems which impair the body’s internal management of insulin and blood glucose. But that’s a complex topic for another time.
Skin
If skin cannot get a good supply of blood, it will have to retreat its resources to the deeper layers that protect organs and sacrifice the superficial layers. This results in patients with diabetes having very dry, fragile, and flakey skin, especially on their feet. It is a common part of the diabetic foot assessment to remove a sock and find a snowbank worth of skin flaking off. I know, it sounds gross, but the body just can’t supply all the layers, so they shed off faster. This also means that the hair follicles die and sweat glands are dysfunctional. The skin also breaks down much faster due to the increased fragility. Again, this results in an increase in risk for wounds, infection, and many other impairments.
And let’s remember that this fragile skin doesn’t have a good blood supply, so when it does eventually break down, blister, get punctured, cut, or burned, it will not heal at a normal rate because it cannot get what it needs.
Muscle, Ligament, Tendon
Muscles have a very high demand for oxygen and nutrients when they are at work, so you can imagine that the muscles in the feet have a high demand often, because whenever a person is standing, those lower legs and feet are working. However, the muscle can’t get the blood flow they need, they cannot contract strong enough or long enough to achieve their task. This ischemia can result in muscle pain. Muscles also produce a lot of waste products from their energy use, and a lack of blood flow results in those waste products building up in the localized region of that muscle. These waste products further damage the endothelium and cause an iterative cycle of damage if left unchecked.
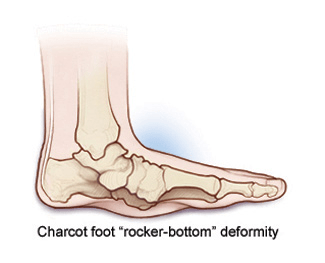
Ligaments and tendons are interesting ones because there is a heavy amount of interaction with the neurovasculature in the function and structure of these tissues and the impact of diabetes on them is clear, but not completely understood. Tendons and ligaments house small organs that perceive many sensations we don’t actively think about, but critically need to stay upright, like kinesthesia and proprioception. The loss of these senses means the ligaments and tendons can’t adjust their tension properly with movement. Specifically in the feet, a loss of ligamentous and tendonous support to the structure of the foot can and will cause serious issues We often see this at its end stages and call it Charcot foot. This is a complex presentation of foot deformity that ultimately results in the collapse of the midfoot, resulting in a rocker-bottom-shaped foot. You can imagine that something like this does not fit well in a shoe.
From a PT perspective, this doesn’t do the patient much good for their gait cycle, either. This foot presentation impairs gait mechanics for several reasons, but the biggest issue is that the patient loses the ability to propel themselves forward with a strong plantarflexor force at toe-off due to altered length-tension relationships in the muscles and tissues and altered joint angles and mechanics. Lack of forward propulsion leads to many biomechanical faults in the gait cycle (hip pain, knee pain, back pain) and can significantly increase the risk of falling. Further, it results in compensations that slow gait speed, which has an overall impact on all-cause mortality. Ya’ll… this is serious. And we haven’t even gotten to the worst part of Charcot foot yet.
Bone
Overall, a lacking neurovascular supply to bone results in impaired bone health and could result in collapse. That is seen in Charcot foot, where the midfoot joints collapse and the navicular literally sits on the ground. This then causes increased pressure (which the patient cannot feel) and often results in ulcers. Other bones are affected, too. Avascular necrosis is more common in patients with diabetes and can impact the femoral head, humeral head, several portions of the tibia, and many other locations in the body. When the bone becomes necrotic, it cannot provide the structural support the body requires, and will often fracture under less stress than normal.
Nails
Toenails are a rough topic for many people with diabetes. Similar to all the other tissues, the nails can not get good circulation. Because they are a protective feature for our foot, they thicken to provide better protection with less supply. This results in nails that are very hard to cut, and often grow in odd shapes and angles. These nails can result in it being very hard to wear normal shoes and further ulcers of the feet can result from improper wear. These toenails also can get infected easier as they collect more debris and don’t receive the immune system warriors as well due to poor circulation.

Where Does Physical Therapy Come In?
So many places!
The foot inspection is a critical part of my evaluation whenever I see a patient with diabetes. Checking for redness, callouses, points of pressure, deformities, circulation, and sensation are all top of my mind. If my patient’s feet are impaired, they don’t have a safe and solid base for movement, so I have to work on that first.
Your first step should be education. Many patients with diabetes don’t know they are having problems with their feet because they can’t feel them. But, if they haven’t lost feeling yet, you can educate them on the signs to look out for and how to delay or prevent these degenerative changes from happening. The education we talked about in Part 1 of this post around managing blood glucose properly, diet, and staying active are key. But there are several more areas we can help.
Break out the hand mirror and start teaching people how to look at their feet! We talked about so many tissues that can be seen from the outside, so have your patient look at their feet every day to inspect for wounds, callouses, signs of pressure, and skin breakdown. Changes in bone structure can be seen from the outside and blood supply can be checked with a simple capillary refill test. Have them clean their feet as part of the process. This may require some special tools but will help prevent infection and callous formation.

Sensation testing is pretty key here. I talked a lot about nervous system testing in this post, but for patients with diabetes, we really want to focus on protective sensation. Break out that monofilament kit and get to poking! Make sure to follow a standardized method (there are lots of options out there), and test both feet! Light touch is great and will tell you a lot about the patient’s ability to detect injury, but don’t forget about other sensations like we talked about earlier. Proprioception and kinesthesia should also be tested and, finally, you should be doing a very thorough balance assessment.
Another great role for the PT performing the foot inspection is to help the patient get shoes! We talked so much in this post about the importance of well-fitting shoes that are to be worn all the time. But patients don’t want to wear shoes all the time if they don’t fit well!. Thankfully, Medicare, and some other payers have agreed and offer patients with diabetes a shoe benefit. Let’s check that out.
Shoes!
In addition to looking at the foot, you also have to look at the shoe. How old is it? How worn is it? Does it fit right? Is it the right size? Does it accommodate swelling? Check out the wear pattern on the bottom and take a peek inside. Pull out the insert and look at the wear pattern on it. Compare that to the foot! Are there areas of redness on the foot that correspond to points of pressure in the shoe? Could the shoe be providing better support for their foot than it is?
Now, let’s get more functional: Can the patient put the shoe on and take it off themselves? Do they need some equipment for that? Can they tie a shoe? Do they need to accommodate an AFO? These are all things we should be thinking about when looking at shoes for patients with diabetes.

Based on Medicare guidelines, patients who are diabetic and meet certain criteria are eligible for a pair of custom/supportive shoes and inserts for those shoes every year. There are some strict criteria around this but there are several roles for us to play in this process. Especially in patients who are homebound or in communal care settings, they may not be able to get out and see a physician for their feet regularly, but we see the folks all the time! So here’s how we can help.
The Medicare criteria for diabetic shoes and inserts require that the patient have a presentation including one or more of the following:
- Previous amputation of the other foot, or part of either foot, or
- History of previous foot ulceration of either foot, or
- History of pre-ulcerative calluses of either foot, or
- Peripheral neuropathy with evidence of callus formation of either foot, or
- Foot deformity of either foot, or
- Poor circulation in either foot
Now, those all sound like things we have already talked about, don’t they? We cannot certify the need for the diabetic shoes under Medicare, but we can notify the physician of the issues and that the patient qualifies based on our physical exam findings. The patient still needs an in-person visit with the doctor at some point, but we can get to that when they are able!

And tell your patient not to worry, they don’t HAVE to get those terrible bulky diabetic shoes if they don’t want to. There are some requirements around what shoes are acceptable, but patients are often able to get a really supportive athletic shoe instead.
Further requirements also talk about a “supplier.” Now, if you are a PT who is also an orthotist, you can be that supplier! Maybe you work for a company that sells diabetic shoes? You can also be that supplier! The supplier is required to perform an assessment for the shoes and assess the fit of the shoes upon delivery and make any modifications necessary to the fit if needed (for those custom-molded pieces).
- Prior to selecting the specific items that will be provided, the supplier must conduct and document an in-person evaluation of the beneficiary.
- At the time of in-person delivery to the beneficiary of the items selected, the supplier must conduct an objective assessment of the fit of the shoe and inserts and document the results. A beneficiary’s subjective statements regarding fit as the sole documentation of the in-person delivery does not meet this criterion.
This is where that team piece comes in. Diabetes impacts every system in the body, so it takes a team to manage it properly. You need someone who can get to the patient, assess their feet, work with you on their specific needs for their mobility, and get the proper devices to the patient as soon as possible to prevent any further injury. Speaking of the team, don’t try to cut those toenails yourself unless you are trained too! Get a podiatrist on board as soon as possible to make sure those feet are in tip-top shape from every angle!
What if You’re Too Late?
I had an amazing patient a long time ago who referred to all his different body parts as car parts. When he came to see me the first time in our little outpatient rural clinic that treated everything, he said he had a flat tire. Turns out his little toe on one foot was black. It was just dead. There was nothing else to it. He had significant vascular damage and neurological impairment due to his uncontrolled diabetes, so he was referred for surgery for him. He talked about losing a lugnut, but it otherwise didn’t bother him much because he couldn’t feel it.
You won’t always get there in time. Know when things can’t be fixed and know when they are beyond your scope and need further care, like antibiotics or vascular surgery.

We will often see a person after their amputation, whether it be a toe, like my friend above, a part of the foot, or the whole foot itself. The goal then becomes to preserve what is left. If the whole foot is gone, do whatever you can to save the other foot. If only the toe is gone, save the others. The higher the amputation goes, the harder the recovery will be, especially considering all the other factors we talked about above that come along with diabetes.
I know it may seem like I’m missing the most obvious piece of the puzzle here (where is the exercise???) but I’m getting to that. Diabetes is a complex beast and there are many places where we fit in. Keep checking back!
What is YOUR role in helping patients get diabetic shoes? Have you had a patient lose a lugnut or other carpart? Tell me in the comments!
Get new content delivered directly to your inbox.
More Reads from the Chronic Disease Management Series









References
Cleveland Clinic Staff. (2019). Charcot Foot. https://my.clevelandclinic.org/health/diseases/15836-charcot-foot
Medicare Coverage Database. (2022). Therapeutic Shoes for Diabetics. Centers for Medicare and Medicaid Services. https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=52501

Follow @DoctorBthePT on Twitter for regular updates!
The contents of this blog and all associated pages reflect the opinions of the author and should not be construed as medical advice. Please consult your doctor for medical advice.
Follow @DoctorBthePT on Twitter for regular updates!
