
If you’ve ever had a student with you for a clinical rotation, you know the feeling of just hoping for that beautiful teaching moment, the one that just opens up naturally. You look for the moment when you can dig a little deeper in to your student’s reasoning skills and let them flex their therapy muscles a little bit harder than usual. It’s one of those moments where they know the right answer, but you get to back track them through the process that they didn’t even know they went through to get there.
I had a wonderful moment like that when I was seeing a patient for at home for sepsis. He had septic pneumonia (same one I mentioned here) and had been intubated and ventilated for several days. He had a complex medical history including DM2, CAD, PVD, and CKD, among other things, but was really just severely deconditioned due to PICS. He came home using a 4-pt walker and 6 L/min of supplemental oxygen. His prior level of function was fishing and doing yard work daily without a device or oxygen. He had rarely ever been sick in his life, and I had the honor of restoring this man to health.
It only took 8 weeks to bring him back and High-Intensity Interval Training was the key factor in his recovery, along with two daughters who ensured 100% compliance with his home program! It was the perfect set up. My student entered on visit number two. She reviewed my evaluation and knew we were going in to a tough case, but she took it in stride. She took charge of his HIIT program and drove the show. Her progressions were beautiful and we worked together to titrate his supplemental oxygen down over time to the point where he no longer even needed it. But the REALLY beautiful teaching moment was the day he came down with gout.
Why on earth would I say gout was beautiful??? It was really the perfect opportunity to integrate her differential diagnosis skills in a patient case that was flowing all too easily. One day, we showed up and our patient couldn’t walk. He was in pain. These things had never been an issue before. We didn’t have a diagnosis of gout at the time, but having seen it plenty of times before, I had narrowed it down fairly quickly. I asked her to do an evaluation of his affected ankle and she did the usual: ROM, swelling, joint mobility… There were some superficial skin wounds so we couldn’t totally rule out cellulitis and she wanted him to see the doctor, so we scheduled him a visit for the next day and we would return the following day for our usual visit.
We got back in the car and I asked her, “so what was your differential list?” I sat and listened quietly as she gave me her list of diagnoses and reasons for each one, but she hadn’t mentioned gout. I attempted to discuss some of the findings with her in relevance to the patient’s age and comorbidities, but still no gout. We discussed it later that day, still no gout. I asked her to go home keep thinking about her findings.

Two days later when we went back, I brought it up on the drive there and asked her if she had changed her mind. She hadn’t come up with anything new and was settled on cellulitis. As we were pulling in to the driveway, I said to her, “it’s gout.” She looked confused and then asked why I thought that. To be completely honest, I should have just said “gestalt” because that was the original reason. But instead, I explained the symptoms in the presence of the patient age and history, and lack of reason for infection (no fever, etc). She nodded and was quietly thinking it over as we walked in to the house.
He had a new prescription for an antibiotic so I was a bit concerned I had been thrown off by an angry cellulitis, but then I asked the patient to tell me about his appointment. He said the doctor told him he couldn’t rule out cellulitis so gave him the antibiotic, but thought it was probably gout. (Phew!)
So, of course, my next step was to ask my student what we could do for our patient to help with his pain and improve his walking while this gout was flaring. Her answer was perfect: ice, elevation, and compression. But wait… what about his medical history? We had just discussed in the car how he had PVD, CAD, and diabetes. I followed her answer with a question, “how do you know it is safe to use compression?” And this is where the teaching moment happened!
I could see in her eyes that she knew where I was going and that not all people can have compression. I could see in her eyes that she even knew the reason I was asking, since we had just talked about his history in the car. But she didn’t know how to know if it was safe. And this, my friends, is where I got to show my student how and why you would perform an ABI. (AND I WAS SO EXCITED!)
ABI stands for Ankle Brachial Index. It is the systolic blood pressure taken at the ankle divided by the systolic blood pressure taken at the brachium. (Ankle over Brachial) An ABI will tell you how well the arteries are able to circulate oxygen and nutrients to the tissues of that lower extremity.
So why would YOU need to do an ABI?
Yes, I said NEED to do. This is for the safety of your patients. You can’t just be throwing compression at everyone who has edema. There is a clinical decision making process that may require further testing before that can be deemed appropriate. Here’s a few reasons to do ABI testing:
- If you are planning on providing compression to lower extremity of a patient with PVD or PAD (or any risk factors for these conditions -see below)
- If you suspect serious PVD/PAD and want to quantify it or monitor progression over longer periods of time (per the Cleveland Clinic, ABI is used for this regularly)
- If your patient is having difficulty healing lower extremity wounds
- Your patient reports increased pain in the legs with elevation which is relieved with dependent positioning
- Your patient reports pain in the legs with activity
This particular test requires some special equipment. I was carrying a Doppler at the time because I had been seeing a couple LVAD patients on and off and needed to be prepared so I retrieved it from my trunk and off we went. If you don’t have access to a doppler, you can use a an automated BP cuff if you are absolutely sure it is accurately calibrated. There is evidence to support this, and it actually increases the specificity of testing significantly.
Speaking of clinometric properties:
When using a Doppler: ABI sensitivity is 95% and specificity is 56% for diagnosis of peripheral artery disease (PAD).
When using an automated blood pressure cuff: ABI sensitivity is 97%, and specificity is 89% for diagnosis of peripheral artery disease (PAD).
Nothing like a good high-specificity AND high-sensitivity test for you to add to your tool box!
As I was having the patient rest in supine for a few minutes to ensure measurement accuracy, I was able to explain the objective findings associated with PAD including:
- Lack of hair growth on the legs
- Skin that feels cold and/or clammy and may be pale or mottled in appearance
- PMHx including diabetes, CAD, high blood pressure, high cholesterol (all of which my patient was on medication for), smoking, and increased age
- Presence of a gangrenous appendage
That last one is a little weird, but I actually did ABI testing on a patient who had a finger that was gangrenous from the DIP distally. It was only one finger, but his ABI was 0.48. His doctor was incredibly grateful for this information and he was scheduled for surgery shortly after, not only to remove the finger, but also to improve his circulation by opening up the vasculature.
How do you do an ABI?
If you can take a blood pressure, you can do an ABI. It does NOT require a special order to be performed. Like I said, you are just taking blood pressures. I’ve taken blood pressure on legs for patients that don’t have arms and I didn’t need an order for that either! However, performing an ABI is a billable service through Medicare, so if you want to get some referrals going for this service, that’s cool, too. (CPT code 93922 (coded twice, once for UEs and once for LEs, typically requires a -59 modifier) and must be in conjunction with a full evaluation or other procedures for reimbursement). (<–DISCLAIMER: I am no coding expert! Please carefully read the descriptions to ensure you are coding properly!)
- Have your patient lay supine and rest for 5 minutes, just like you would if you were doing orthostatics.
- Take their normal brachial blood pressure and record your number.
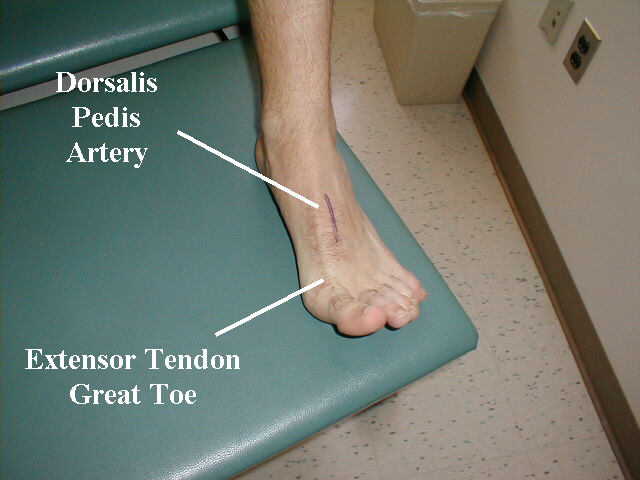
- Take out your Doppler and find that dorsalis pedis artery (or posterior tibial).
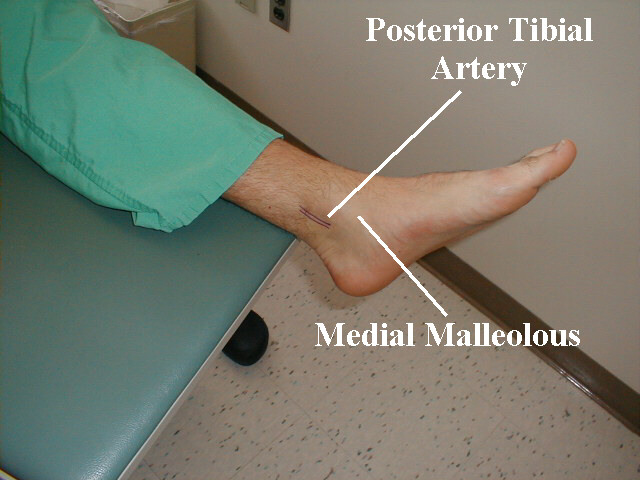
- Get the cuff of your patients leg and inflate until you no longer hear the dorsalis pedis, then go up another 20 mmHG just like you should when taking a typical blood pressure.Release the pressure slowly (just like normal) and record your systolic result (the number at which you hear the dorsalis pedis/posterior tibial flow return).
- Repeat on the other leg and then arm.
- Divide the highest ankle systolic by the highest brachial systolic to get your result (See worksheet)
To make your math even more simple, you can download this worksheet from Project Lead the Way (2014):

Or if that doesn’t work, there is a comprehensive worksheet and instruction set here.
Ok…. so now what?
Well, there are some normative values to which you need to compare your result
- Normal: 1.0 to 1.3
- Borderline PAD: 0.9 to 1.0
- PAD: 0.9 or less
- Moderate PAD: 0.4 to 0.7
- Severe PAD: less than 0.4
- If you get a number greater than 1.3, this indicates the arteries have become rigid. Arterial calcification is typically at fault, thanks to diabetes.
If you are seeing numbers in the severe category, you can anticipate this patient needing some more extensive interventions IF they are medically stable enough to receive them. However, if their vasculature is functioning that poorly, they may not be stable enough. They would also NOT be a candidate for use of compression to treat whatever it is you are looking to treat, as they would be at a significantly increased risk of losing complete blood flow to their extremity. Needless to say, this should mean you are calling the doctor.
It should be mentioned that it is not your role to interpret ABI information. You can and should be assessing this information, but it is the physician’s call about what to do with it, so report it! Just like with orthostatics, this information is very important in the overall clinical and medical picture of the patient, so doctors want to know!
Thankfully, our patient was giving us 1.1 and 1.2 so he was not at risk for adverse events with proper use of compression. We utilized an ACE wrap and his daughter bought him some low level compression stocking which worked beautifully once we showed them how to put them on him. His gout was fleeting, only a few days, and he was back on track in no time.
How often do you treat patient who have PAD? What interventions do they typically benefit most from? Tell me about it in the comments!

Pressure… Pushing Down On Me…
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…

Dehydration
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease

Chronic Disease Part 3: Urinary Incontinence – Part 1
NEXT FEATURE IN THE CHRONIC DISEASE MANAGEMENT SERIES!!!
Let’s learn how to manage incontinence! But wait, that’s not a chronic disease, is it? Well, let’s take a look and find out!
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!
References
Chaudru, S., de Müllenheim, P. Y., Le Faucheur, A., Kaladji, A., Jaquinandi, V., Mahe, G. (2015). Training to Perform Ankle-Brachial Index: Systematic Review and Perspectives to Improve Teaching and Learning. European Journal of Vascular and Endovascular Surgery. 51. 10.1016/j.ejvs.2015.09.005.
Cleveland Clinic. (2019). Ankle Brachial Index. Retrieved from https://my.clevelandclinic.org/health/diagnostics/17840-ankle-brachial-index-abi
Crawford, F., Welch, K., Andras, A., & Chappell, F. M. (2016). Ankle brachial index for the diagnosis of lower limb peripheral arterial disease. The Cochrane database of systematic reviews, 9(9), CD010680. https://doi.org/10.1002/14651858.CD010680.pub2
Herráiz-Adillo, Á., Cavero-Redondo, I., Álvarez-Bueno, C., Martínez-Vizcaíno, V., Pozuelo-Carrascosa, D. P., & Notario-Pacheco, B. (2017). The accuracy of an oscillometric ankle-brachial index in the diagnosis of lower limb peripheral arterial disease: A systematic review and meta-analysis. International journal of clinical practice, 71(9), 10.1111/ijcp.12994. https://doi.org/10.1111/ijcp.12994
Jitendra, M. (2020). Medical Coding Guide: Tips for Coding ABIs. American Medical Coding. Retrieve from https://www.americanmedicalcoding.com/tricks-to-code-cpt-code-93923/
National Institutes of Health. (2020) National Heart, Lung, and Blood Institute: Peripheral Artery Disease. Retrieved from https://www.nhlbi.nih.gov/health-topics/peripheral-artery-disease
Project Lead The Way. (2014). Human Body Systems Activity 4.3.5 Student Resource Sheet. Retrieved from https://www.scribd.com/document/349521701/4-3-5-a-sr-abi-worksheet

Follow @DoctorBthePT on Twitter for regular updates!

{kind=link}
One thought on “That Beautiful Teaching Moment: ABI”