
So now that you know how I feel about primary care PT, you need to know that this ties very closely with my practice. I have extensive experience in the treatment and management of patients with chronic disease. And when I say the treatment and management, I don’t mean that I went to their house and gave them some exercises, then left the rest to my (very skilled) assistant to handle until discharge. I mean that I saw them for a skilled home evaluation where we discussed the impact of their comorbidities on their life and function, performed evidence-based tests and outcome measures, and then created a care plan that included the patient’s goals as well as lifestyle modifications and education to control their diseases. Let’s be real: our profession is not following a protocol.
That means that there were evaluations where I talked about nothing but going to the bathroom safely and successfully. There were visits where I performed one single intervention for breathing (active cycle of breathing) and it took an hour. There were discharges that became reassessments because the patient started showing changes in their lung auscultation (new onset pneumonia). There were patients I saw for one diagnosis (a clavicle fracture) but treated and referred for another (undiagnosed Parkinson’s Disease). Sometimes I didn’t perform any interventions with the patient at all, but spent an hour with the caregiver trying to work things out. I have even spent an entire evaluation doing diabetic teaching on how to use a glucometer properly.
The chronic diseases I frequently treat include diabetes, congestive heart failure, chronic obstructive pulmonary disease, organ transplant (heart, lung(s), kidney, liver…), incontinence, hypertension, coronary artery disease, frailty, osteoporosis, chronic kidney disease, and end stage renal disease. I do not claim to be a neurological clinical specialist, but I do focus on the cardiovascular impairments associated with neurological conditions including orthostatic hypotension associated with Parkinson’s Disease, the vascular and cardiac impairments that cause cerebrovascular accidents, and the sequelae of falls such as bleeding (internal or external), brain injuries, and vestibular dysfunctions. And after COVID-19, we may even see a whole new subclass of chronic disease that we need to be addressing! Post-COVID syndrome, maybe?
Yes, I see total knee replacements, but I also see the chronic smoking that will delay healing due to intermittent tissue hypoxia and increased risk for infection. Yes, I see shoulder impingement, but I also see the eye aversion and reports of constant fatigue indicating depression and need for referral. Yes, I see low back pain, but I also see the urinary incontinence that so often is copresent and fully treatable.

Did you know that the things you can do as a physical therapist to help manage and treat chronic disease are so small and so easy that you probably have just overlooked them? Let’s talk about those things:
- Ask about medications. I don’t mean asking if they take any. Yes, that is important, too, but ask if there have been any recent changes to their medications or if they started or stopped a medication lately. I have treated a patient for falls that happened because she was snowed on psych meds. Once we worked with her doctor to cut her dosage in half, she stopped falling.
Most importantly, ask if your patient has taken their medications today!!! I cannot even count the number of times I have taken a blood pressure before starting a session to find severe hypertension and when I asked if the patient took their meds today, the answer is always “no, I forgot…” The only thing that tops that is how many times I have found severe hyperglycemia. Medication compliance is terrible generally with chronic disease, but, to be more specific for you:- Patients with type two diabetes are noncompliant with medications up to 81% of the time.
- Patients taking medication for hypertension are noncompliant as often as 30% of the time.
- Ask about incontinence. Everyone will deny they have it so you need to find another way to ask. “Do you ever have any leakage when you cough or sneeze?” “Do you ever need to use incontinence products?” “Do you ever have to change your clothes mid-day due to leakage?” If you don’t get specific, you won’t get a useful answer. 80% of women and (possibly up to) 60% of men have some type of incontinence at some point in their lives. You may catch them as that point. Stress, urge, functional, and mixed incontinence can be fully treatable if you know they exist. We also know that urinary incontinence and constipation have a strong correlation with low back pain. If you can address either issue or both, back pain has a good chance of improving or being relieved. This is coming from someone who utilizes a fully mechanical approach to back pain like 90% of the time…
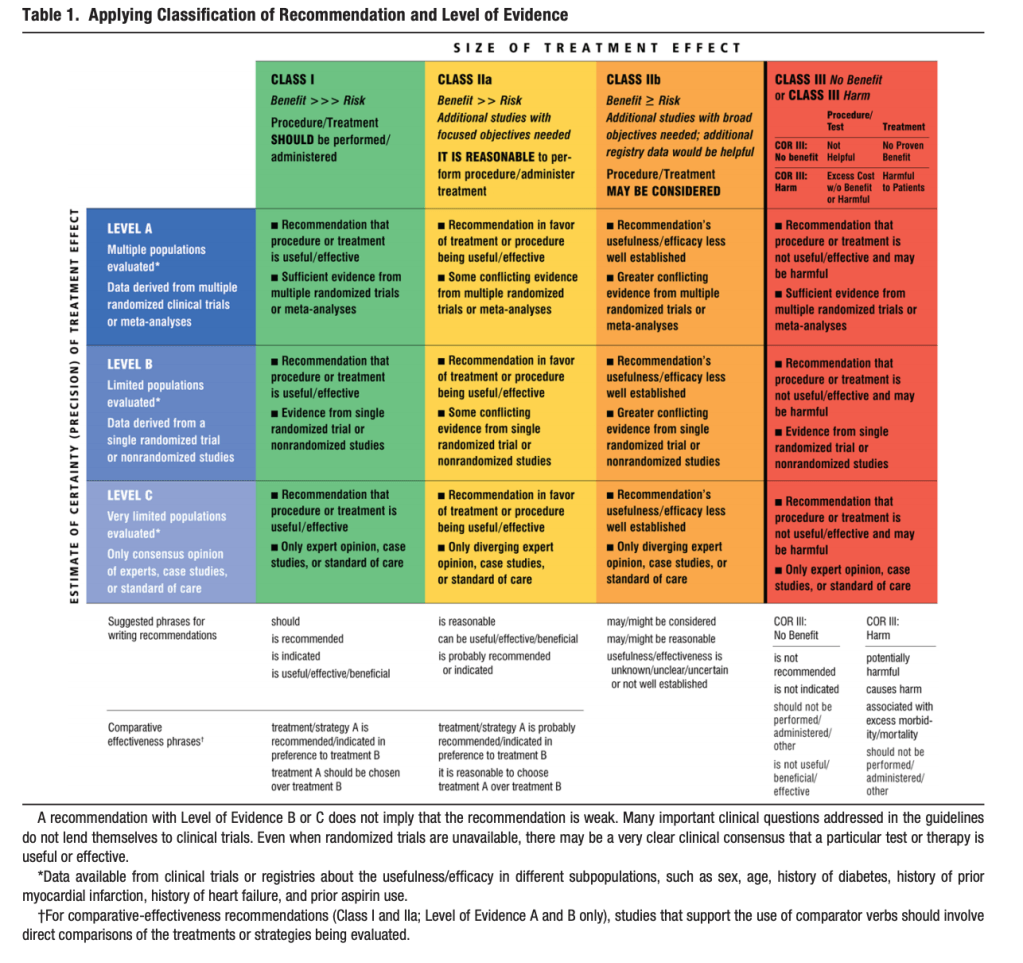
- Take Vitals. I should really just stop there… but I won’t (Ha! You should know me enough by now…). If you don’t know where you started, you don’t know where you’re at. If you take a blood pressure midway through your session, hey, that’s great! But that number doesn’t carry much weight if you don’t have something to compare it to. In the home care setting, when I have students, I always discuss with them the impact of chronic disease. I ask them, “How can you know if your patient is safe to get up out of their chair, today?” The answer is vitals. Not in the home care setting? Fine. Take them anyway. 90% of the time, you’ll see great numbers and everything will be fine, but that 10% is the part that matters. You may think you are pretty good at identifying people at risk for high blood pressure based on presentation. There is research to show that we are pretty good at figuring out who is really high risk and who is really not, but what about all those people who only have some risk factors (aka most of your patients)? If you need some guidance on those risk factors, the American Heart Association has constructed this table:
- Weigh your patients. This may sound a bit strange, but isn’t exercise one of the best treatments for just about everything including obesity? We know this. This isn’t new. Taking your patient’s weight can also be really helpful to track trends over time. But in the chronic disease management world, taking daily weights is necessary for management of congestive heart failure. (We talk more about that here!) It can also be really helpful when treating patients who undergo renal dialysis as fluid load directly impacts their ability to participate in physical therapy. Teaching your patient how to safely step up on and down from a scale is billable. Teaching your patient the importance of daily weights for preventing exacerbation is billable.
- Blood glucose monitoring. Your ability to do this may vary based on your state, but we all know the importance of blood glucose for exercise. If we don’t time our sessions properly, we end up with a patient passing out on us. If we do time them properly, we can actually (over time) decrease or eliminate the need for medication to manage blood glucose. Let’s talk about the logistics of this:
- To clear up the risk analysis: If your patient is already diabetic, they already have a physician’s order to check their blood glucose daily. If you ask them to or assist them in doing this prior to your session or during your session, you are in full compliance with this order. If you need to do this for your patient because they are unable, you are still in full compliance with this order. If your patient’s blood glucose is so low that they are fully unable to take their glucose themselves, are you going to sit there wondering if its ok while they fade away? No, of course not. You should probably be calling 911 at that point, but take their blood glucose. (Side note: please wear gloves.) Diabetic teaching is well within our scope of practice. So is diabetic intervention (aka exercise). PTs can even become certified diabetic educators.
- You cannot administer insulin if your patient’s blood glucose is too high unless you are trained to use the devices to do so and there is an order in place (if your patient is diabetic, there is an order in place, but you have to know how much, i.e. sliding scales and all that). You should be calling the physician for instruction if your patient cannot self-administer. You can, on the opposite end of the spectrum, give your patient food. You should have fast-acting sugars available in your clinic: juice, candy, applesauce… Even in outpatient clinics, I’ve given juice when I noticed the signs of hypoglycemia.
- What are safe parameters for blood glucose? I thought you’d never ask 🙂
Too low: <50 mg/dL call physician/911 based on symptoms
Too low for exercise: <70 mg/dL give sugar
IDEAL RANGE: 100-250 mg/dL
Too high for exercise: >250 mg/dL call physician, risk of ketoacidosis
Too high: >350 mg/dL call physician/911 based on symptoms
***If doing an exercise class or performing exercise in long bouts (longer than 60 minutes) blood glucose should be checked every 30 minutes to ensure ongoing safety.
Ya’ll, that’s it. Really. All of these things are easy, quick, and well within our scope of practice. If we are claiming to provide primary care (which we definitely claim to do and actually do all the time!), we need to do the things that go along with it. You may be thinking that, even if these things are quick and easy, you can’t afford the extra minutes. When exercising someone with a chronic disease, you can’t afford not to spend the time. It could literally mean life or death in some cases. You may find out some surprising things! Maybe they’ve been struggling with loading needles in to their lancet device, and there’s an opportunity for some education and functional training.
The future of our profession may be providing exercise as an intervention for people with all kinds of chronic diseases like anxiety or depression. We already treat cancer and chronic pain. We need to be treating obesity and hypertension as a primary intervention. It will not be long before we are providing interventions for the prevention of a stroke based on a patient’s risk factors, so you better be good at taking blood pressures. Exercise prescription based on your genetic profile is already on its way where we will be able to predict the risk of a cardiovascular event at different intensities. You may even need to start incorporating a patient’s social determinants of health in to your plan of care if you haven’t already. Are you ready for this?
Well? Are you ready? Tell me how in the comments!


















Follow my blog for more!
References
Goff, et al. (2014). ACC/AHA Guideline on the Assessment of
Cardiovascular Risk: A Report of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines. Circulation. Retrieved from https://www.ahajournals.org/doi/pdf/10.1161/01.cir.0000437741.48606.98
Hedegaard U, MS, Kjeldsen, Lene Juel, MS, PhD, Pottegård, Anton, MS, PhD, et al. Improving medication adherence in patients with hypertension: A randomized trial. Am J Med. 2015;128:1351-1361.
Mayo Clinic. (2020). Diabetes and exercise: when to monitor blood sugar. Retrieved from https://www.mayoclinic.org/diseases-conditions/diabetes/in-depth/diabetes-and-exercise/art-20045697#:~:text=You’re%20good%20to%20go,too%20high%20to%20exercise%20safely.
Polonsky W, Henry R. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence.. 2016;10:1299-1307.

Follow @DoctorBthePT on Twitter for regular updates!

8 thoughts on “Expanding Your Role, Fulfilling Your Scope”