
I was seeing a younger man in the home setting after a CABG x3 procedure. When I evaluated him, I was a bit frustrated because he had impaired cognition and had significant comorbidities for a younger man, none of which was in his referral information. Instead, I had the pleasure of just picking up on these things as I went along through my evaluation. His caregiver was reporting to me that he was very fatigued, very confused, very not himself since the surgery. He was a smaller man and did not seem to be exhibiting any signs of fluid overload. So I went on to what I typically look for in a patient immediately after CABG: orthostasis. In my article about Beta Blockers, we discussed how these medications are typically prescribed along with other medications after CABG procedures and this frequently results in orthostasis.
I began to perform the standard four-position orthostatic assessment that I mentioned in those posts and found him to be significantly orthostatic, to the point where I could not stand him up for more than a few seconds before he just sat down on his own due to being “lightheaded”. This seemed a bit extreme, but he was also likely dehydrated. However, yellow flags were going up in my head. I decided to investigate further. I noticed when taking his pulse and blood pressure that his heart rhythm was irregular so I took an extra listen to the main equipment.
La – Da – Da – La – Dub… Uh Oh.
This man’s heart sounded like an engine misfiring on all cylinders. There was some serious electrical disturbance going on here. I could hardly make sense of the sounds I was hearing. I contacted the cardiologist’s office and reported my findings (which probably sounded like I was completely unable to auscultate heart sounds… “uh, your patient’s heart isn’t demonstrating a typical contraction pattern upon auscultation…” was the best I could do without sounding just foolish).
Thankfully, his primary nurse arrived shortly after I discovered these findings and we had the opportunity to talk it over and attempt to figure it out. Ultimately, we decided he needed to go in and he was admitted.
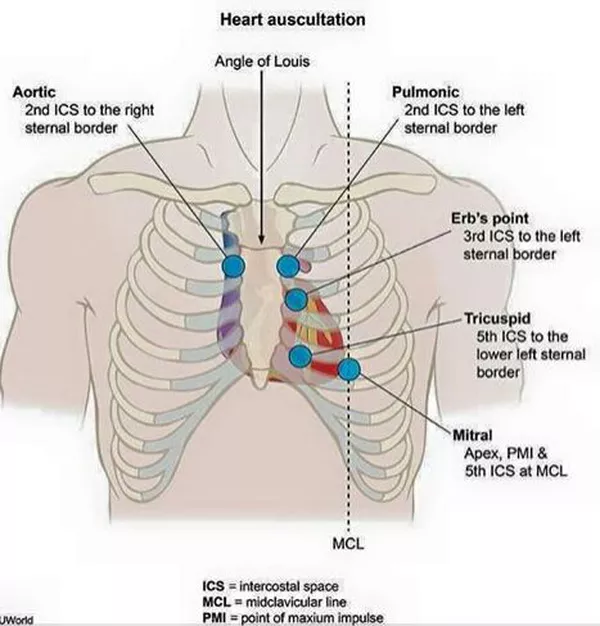
So let’s take a look at heart auscultation. There are two main methods to do this, but, for the sake of simplicity, I’m just going to discuss this one. The “All Physical Therapists Move” method (also known as the “All Physicians Take Money” method) is the easiest to remember what you are actually listening to.
All. A is for Aortic Valve. Auscultating this structure will need to be done over the right second intercostal space at the sternal border. This is your “Dub”.
Physical. P is for Pulmonic Valve. Auscultating this structure will require you to place your stethoscope at the left second intercostal space, also at the sternal border. This is also your “Dub”.
Therapists. T is for Tricuspid. To auscultate this structure, place you stethoscope in the left fifth intercostal space, just lateral of the sternal border. This is your “Lub”.
Move. M is for Mitral (Also known as Bicuspid). To auscultate this structure, place your stethoscope in the left fifth intercostal space at midclavicular line. HOWEVER, this can be difficult to do with some female patients, and auscultation of sound may be difficult if the patient exhibits a bariatric build. So it can be easier to auscultate this valve at the same level, but at the midaxillary line. I typically perform this auscultation in this manner. This is also your “Lub”.
Next you need to know what you are listening for. There are four common heart sounds: S1, S2, S3, and S4. You really only want to hear two of them (S1 & S2), but sometimes you get a third or fourth thrown in. This can mean absolutely nothing, or it can mean poor cardiac function. It depends on the patient.
S1. “Lub” This is the normal sound of the Mitral and Tricuspid valves closing.
S2. “Dub” This is the normal sound of the Aortic and Pulmonic valves closing.
S3. An abnormal sound heard shortly after S2. It typically indicates delayed ventricular filling. This can indicate heart failure in some patients.
S4. Another abnormal heart sound heard shortly before S1. This sound tends to be more problematic as it indicates significantly delayed ventricular filling. This sound is regular associated with coronary artery disease, aortic stenosis, hypertension, or a heart attack.
***HOWEVER, in athletes, an S4 can be normal as it can indicate very efficient cardiac function or physical changes to the heart structure due to training (known as Athlete’s Heart). It is important to distinguish between this and serious clinical pathology. Athlete’s heart is a particular collage of findings including systolic murmur, S4 gallop sounds, and bradycardia in an asymptomatic and well-trained patient. Up to 1/3 of athletes have various electrical rhythm anomalies, some that occur only during exercise, and this can be completely normal. However, symptoms can be similar to hypertrophic cardiomyopathy so cardiac workup is warranted. Typically only an ECG is needed.***
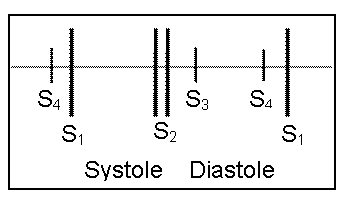
So what are these sounds telling us? The closing of these valves is in precise timing, only about 0.1 second between S1 and S2. So if we are hearing other sounds, the timing is off. Similar to a car engine, this means bad things are probably coming. Extra sounds indicate electrical anomalies that can be seen on EKGs. So what does normal electrical heart function look like?

The usual path looks like this:
Sinoatrial (SA) Node –> Atrioventricular (AV) Node –> Bundle of His –> Atrioventricular (AV) Bundle –> Purkinje Fibers
But many different things can throw a wrench in to this system. In my post on beta blockers, I talked about atrial fibrillation which is just one of the many rhythm disorders we can see. I’m not going to pretend to know more about the electrical function of the heart than a cardiac nurse, so I’m going to let him give you this really awesome explanation. He also goes in to the easy way to read and interpret EKGs. His description makes this so easy to understand so I highly recommend watching it!
As a rehab clinician who is working in most settings, you don’t have to know ALL the details. What you do need to know is what is normal. That way, when you come across something abnormal, you can identify it and make sure it is addressed by the appropriate person. So, just like I recommend when it comes to lung auscultation, just start listening to everyone’s heart! Patients don’t know the different between listening to their heart and listening to their lungs so just listen to it all while you are there. Get an understanding of the variations on normal and try out different auscultation spots like I mentioned above. Soon, you’ll be identifying abnormal sounds and maybe even saving a life by early detection. You’ve got the skills!
Have you ever heard a crazy set of heart sounds? Or listened to heart sounds on something other than a human? Tell be about it in the comments!
More from the Pulmonary Rehab Toolbox…

Airway Clearance Techniques
SAVED THE BEST FOR LAST! COPD Management bonus content is here and it’s a special treat fo you!

Pulse Oximetry and O2 Saturation
SO MUCH BONUS CONTENT! One of my favorite posts on COPD management – Let’s go for a ride down the river…

Spilling the Box of Pearls: All the Tips on Supplemental Oxygen Management
Can’t get enough BONUS CONTENT! Still managing COPD but struggle with the oxygen? I’ve got you…
Something went wrong. Please refresh the page and/or try again.
Follow my blog for more!
References
Magic In Nursing Team. (2017). EKG/ECG Interpretation (Basic): Easy and Simple!. Retrieved from https://www.youtube.com/watch?v=FThXJUFWUrw
McKelvie, R. (2019). Athlete’s Heart. Merck Manual: Professional Version. Retrieved from https://www.merckmanuals.com/professional/cardiovascular-disorders/sports-and-the-heart/athlete%E2%80%99s-heart on 6/22/20.

Follow @DoctorBthePT on Twitter for regular updates!

9 thoughts on “The (Very) Basics of Heart Auscultation”