
Let’s talk about this super simple technique that can change everything. Diaphragmatic breathing is really just how we are all supposed to be breathing most of the time. The purpose of the diaphragm is to facilitate breathing. Diaphragmatic breathing improves gas exchange and increases lung volumes. These are all really good things if we need to get more air in, such as in restrictive lung diseases like pneumonia, post-lung resection, or pulmonary fibrosis. It can also be a useful technique to mobilize secretions or other obstructions in the airway for people who have obstructive lung conditions like congestive heart failure or COPD.
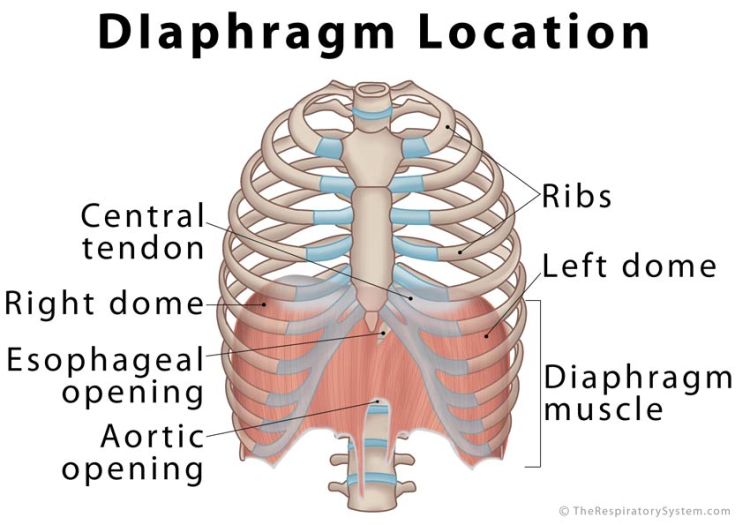
It can be a bit difficult to grasp the actions and movements of the diaphragm unless you understand its purpose. The diaphragm has a central tendon and attaches to the costal margins, spine, and xyphoid process to create a barrier between the thoracic cavity and abdominal cavity. There are openings in the diaphragm muscle (hiatus) for the passage of the major blood vessels (the descending aorta and inferior vena cava), the trachea, the esophagus, and a few other small circulatory structures.
As you can see in the picture, when this muscle is relaxed, all of its length is up inside the chest cavity. Per the standard skeletal muscle, when it contracts and the fibers shorten. This brings the insertion (the central tendon) to the origin (the costal margins, spine, xyphoid). The central tendon lowering down into the abdomen, increasing the volume of the thoracic space to allow for lung expansion and decreasing the volume of the abdominal space. There are other accommodations that happen to make up for this volumetric change, but we will talk about those in a different post.
Because of the negative pressure system within our pleural space, this increase in thoracic volume draws air into the lungs, allowing for increased ventilation and diffusion (aka gas exchange) to take place, specifically in the lower segments of the lungs. This allows for greater oxygen intake and great CO2 removal, or more efficient breathing, than if the diaphragm were not engaged during this task. Breathing that does not engage the diaphragm utilizes the upper intercostals and accessory muscles to open the upper portions of the lungs only for gas exchange. This is less efficient and is typically seen in patients who have chronic heart and lung diseases or spinal cord injuries.
Why do we stop breathing the way we should?
Well, there are many reasons. Skinny jeans, corsets, getting our picture taken, learned habits, sitting without a back support, spinal deformations, pain avoidance, central nervous system damage, gastrointestinal disturbances, space-occupying lesions, change in muscle strength or length (disuse atrophy or trigger points can come in to play here), changes in abdominal content volume (pregnancy or obesity), change in lung volume (resections), lung function changes (disease states)… the list is endless. The major factor is whether or not it becomes a persistent problem. The body is a smart system and it can compensate for pretty much anything, but, similar to other musculoskeletal impairments, long term compensations are what lead to problems.

What can we do about it?
Bring it back! The diaphragm may shut down for a number of reasons, but it can bounce back with pretty minimal input. The reason for that is because it is such an essential muscle! It utilizes three spinal levels to ensure its function (C-3, 4, 5, Stay Alive!) because redundancies ensure we can breathe, at least in part, even if there is some damage.
The reason we had to talk about all that old information about origins, insertions, and actions is because these things are going to be important when attempting to facilitate diaphragm function. We used to teach people to have patients lying in hooklying with an object of interest (TV remote, cell phone) on their abdomen. We would ask them to breath inward and use their air to raise the item on their abdomen. When the diaphragm contracts to compress the diaphragm, the contents have to go somewhere and that is usually outward, so the object rises. BUT HERE’S THE PROBLEM WITH THAT: The diaphragm doesn’t move that way! These techniques typically result in the patient performing a Valsalva maneuver.
The diaphragm doesn’t move up and down when in the hooklying position! It moved cranial/caudal, which is completely different. The diaphragm attaches all the way around our body (nearly 360 degrees), so we need to be facilitating it’s expansion all the way around, also! We can’t do that if someone is lying on their back for many reasons:
- This applies resistance to the posterior segments of the diaphragm muscle, making it harder to activate all portions of the muscle.
- The diaphragm needs to work in 360 functional space including all positions of the body! So diaphragm exercises need to be performed in sitting, standing, squatting, quadruped, laying, and whatever yoga pose you come up with next.
There is a small case for initially instructing diaphragm exercise in hooklying, because this allows for gravity neutral activation, but you better move on pretty quick if your patient is ambulatory and doesn’t have a high spinal cord injury, or you won’t be doing them any good.

What does diaphragm facilitation look like?
There are many ways to facilitate diaphragm activation but here are some I like to use:
- Visual Feedback: Place the patient in a chair in front of a mirror and have them breathe in and out using their diaphragm. Do this with them so they can see what you look like as well.
- Verbal cues:
- “Breathe in deeply, bringing the air all the way down to the bottom of your lungs”
- The “Triple Sniff”: Ask your patient to sniff quickly three times. The first two sniffs need to be short and the third one needs to be long.
- Manual Facilitation: Place hands all the way around the patient! We cannot cue diaphragm breathing in one plane because that’s not how it happens so here are some options:
- Basic: one hand on chest, one hand on abdomen – abdomen should raise equal to or more than chest with inhalation (not my favorite as it results in Valsalvas more times than not).
- Better: Place C-shaped hands around the inferior costal margin bilaterally. Ask the the patient to breathe in to your hands.
- Best: With your C-shaped hands, follow that inferior costal margin inward on the exhale and provide a deep quick stretch just before the inhale to cue diaphragm and lower intercostal muscle activation.
When utilizing manual facilitation, you will want to make sure you feel all margins of the insertion expanding and contracting so you may have to facilitate from several different points on the costal margin over several repetitions.
Any other tips, Doctor B?
The diaphragm works in concert with the pelvic floor. Make sure your patient doesn’t have to use the bathroom and isn’t tightening their pelvic floor again exhalation. This results in over-compression of the abdominal contents and result in prolapse or incontinence. This is especially a concern for female athletes, new mothers, and women who have chronic breathing problems. 55% of women without a chronic lung disease reported incontinence, whereas 71% of women with a chronic lung disease reported incontinence.
Female athletes (I’m looking at you, gymnasts!) can also use many other muscle systems to facilitate breathing and compensate for their diaphragm. Be sure to check out breathing with the scapulae and even the glutes! This can have serious implications for the pelvic floor, also.
Patients who have spinal cord injuries, or some degenerative neurological conditions such as MS, GBS, or ALS may have partially impaired diaphragm function and will require several different types of facilitation. Just like airway clearance techniques, these interventions are always best performed in addition to each other, not in isolation.
Patients who have chronic diseases that results in poor lung function, like we mentioned above, typically need to get more air OUT of their lungs before putting more air INTO their lungs with diaphragmatic breathing. Check out this post on dynamic hyperinflation to learn more about that. You may also find that facilitating diaphragmatic breathing results in expectoration of secretions for patients who have obstructive lung conditions. This is because they are finally getting some ventilation to these no-often-used parts of their lungs! Alternating techniques that remedy dynamic hyperinflation with diaphragmatic breathing, as well as providing some positive expiratory pressure can make fore a really useful set of exercises for someone who has impaired lung function, but make sure you get the order of operations correct!
Do you have any funny verbal cues you like to use for diaphragm retraining? Tell me about them in the comments!

Pressure… Pushing Down On Me…
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…

Dehydration
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease

Chronic Disease Part 3: Urinary Incontinence – Part 1
NEXT FEATURE IN THE CHRONIC DISEASE MANAGEMENT SERIES!!!
Let’s learn how to manage incontinence! But wait, that’s not a chronic disease, is it? Well, let’s take a look and find out!
Something went wrong. Please refresh the page and/or try again.
References:
Button, B. M., Holland, A. E., Sherburn, M. S., Chase, J., Wilson, J. W., & Burge, A. T. (2019). Prevalence, impact and specialised treatment of urinary incontinence in women with chronic lung disease. Physiotherapy, 105(1), 114–119. https://doi.org/10.1016/j.physio.2018.07.006
Lee, D. (2019). Butt-grippers, Back-grippers and Chest Grippers. Retrieved from https://dianeleephysio.com/education/butt-grippers-back-grippers-and-chest-grippers/

Follow @DoctorBthePT on Twitter for regular updates!

One thought on “Diaphragmatic Breathing”