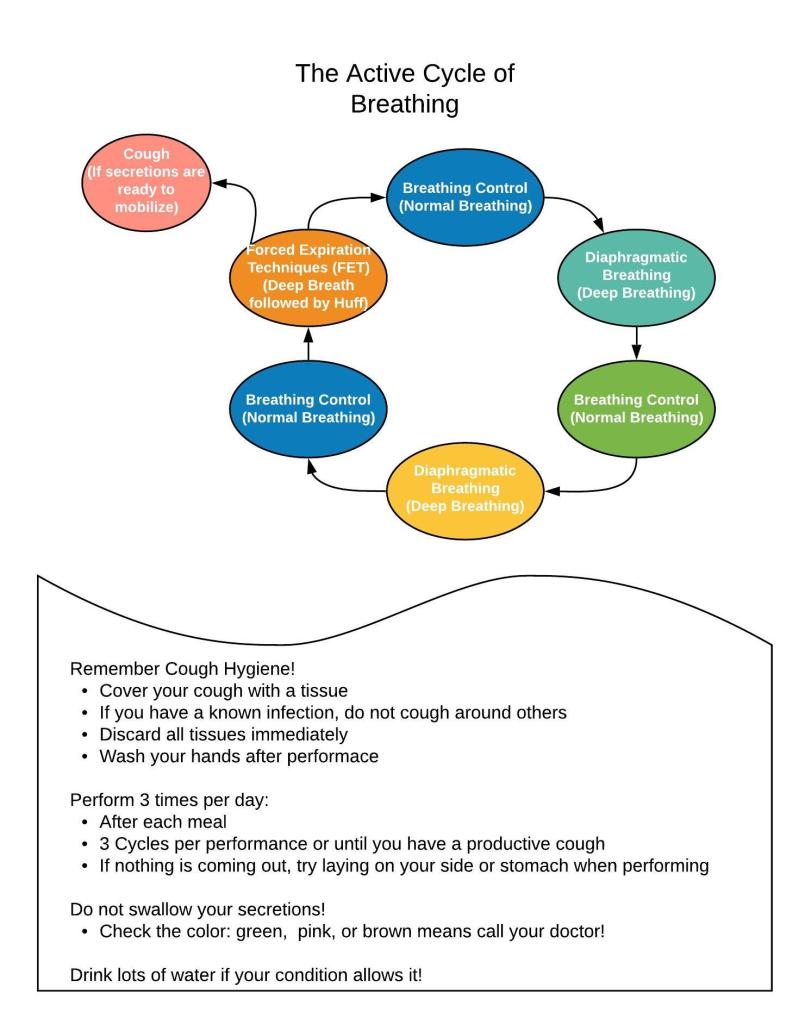
The Active Cycle of Breathing is a critical tool for secretion mobilization. It can also be modified in several ways to address patient-specific needs. But the basic cycle is more than enough for most patients. The goal is to loosen secretions and get air underneath them so they can be mobilized (or coughed) out.
I teach this to my patients pretty often across multiple settings, but there are a few things specific to COVID-19 that we need to remember:
These patients have an active viral infection that is easily spread
Others in the room may be at risk so the patient should only be performing this in a closed room
Performance of the ACBT with a COVID-19 patient put YOU at risk, especially if you do not have the proper PPE
HAND HYGIENE IS CRUCIAL
As COVID-19 is a restrictive disease state, you may not need airway clearance techniques. But that doesn’t mean you won’t need many other interventions.
I thought this post would be a little more entertaining if you guys had a video so here goes…
I’ve provided you with a downloadable printout to hand to your patients when you are instructing this. I have also not included any reps or times on this hand out so that you can change it for your specific patient tolerance. I’ve found that my home care patients could typically tolerate 5-10 reps of each activity around the cycle, but my SNF patients max out around 5. That original cycle recommends 20-30 seconds at each activity, but my patients simply can’t do that most of the time. The overall recommended duration of performance is 10 minutes.
How did your patients like the handout? What modification do you find yourself making most often as you instruct this intervention? Let me know in the comments!
Home health care PTs are incredibly familiar with the term “homebound.” It determines whether or not we can provide home-based services to a Medicare patient. Directly from CMS…
“Home health services are or were required because the individual is or was confined to the home per the criteria below (as defined in sections 1835(a) and 1814(a) of the Social Security Act).
a. Criteria-One: The patient must—
Because of illness or injury, need the aid of supportive devices such as crutches, canes, wheelchairs, and walkers; the use of special transportation; or the assistance of another person in order to leave their place of residence – OR –
Have a condition such that leaving his or her home is medically contraindicated. If the patient meets one of the Criteria-One conditions, then the patient must ALSO meet two additional requirements defined in Criteria-Two below.
b. Criteria-Two:
There must exist a normal inability to leave home; – AND –
Leaving home must require a considerable and taxing effort”
Now, interpretation of homebound is pretty open, even though it probably isn’t supposed to be as flexible as it is typically applied. CMS Link
The way I was taught to look at it is this:
Homebound is not a choice, it is a condition. You either have it or you don’t.
However, this has all just changed. CMS has updated the definition of “homebound” to increase their flexibility in fighting or preventing COVID-19. The new definition allows for quarantine status to be included as well as a diagnosis of COVID-19. The new definition also includes patients who would be considered by a physician as being at “high-risk” for contracting COVID-19 if they left the home.
The new definition is as follows:
“A beneficiary is considered homebound when their physician advises them not to leave the home because of a confirmed or suspected COVID-19 diagnosis or if the patient has a condition that makes them more susceptible to contract COVID-19. As a result, if a beneficiary is homebound due to COVID-19 and needs skilled services, a HHA can provide those services under the Medicare Home Health benefit.” CMS Link
One of the biggest changes also included in this new document is that agencies or clinicians are allowed to perform initial assessments, determine appropriateness, and screen homebound status via remote video or recorded video!
Medicare has been restricted in the realm of telehealth due to statutory confinements, so this particular change is significant.
The new changes also allow for increased OASIS transmission time, POCs to be supervised by NPs and PAs.
For a full rundown of the changes allowed by this new document, check out the link.
How do you feel the change in the definition of “homebound” will impact your safety as a home health provider? Let me know in the comments!
Breathing. I can’t stress it enough. If you’re not breathing, you’re dead… or in a lot of pain… either way, it’s not good. So breathe! In my practice, I work with a lot of different types of patients with a wide variety of conditions and comorbidities, but they all have one thing in common: they…
WHILE WE WAIT FOR THE NECT CHAPTER OF DIABETES MANAGEMENT, LET’S KEEP TALKING ABOUT INCONTINENCE
Chronic management of urinary incontinence can lead to many issues like infection and hospitalization if it doesn’t account for fluid balance! Let’s talk I’s and O’s! #physicaltherapy #incontinence #chronicdisease
It is thought that the IS is used to reduce the risk of post-operative pulmonary complications (PPCs) by increasing total lung inflation, tidal volume, and vital capacity.
What Does the Evidence Say?:
The most current evidence DOES NOT support the use of incentive spirometry for any patient as a first line intervention to prevent or decrease risk of PPCs or improve pulmonary function.
Early mobilization, Diaphragmatic breathing exercises, and active cycle of breathing have also been shown to decrease risk of PPCs better than IS with no benefit of addition of IS to these interventions.
Post-CABG and post-abdominal surgeries of all kinds were the primary populations studied with highest level evidence. Moderate level evidence in the same persuasion was given for post-trauma and cancer patients. Current evidence also reports poor compliance with IS performance.
The IS has not been shown to be effective for patients being treated for COVID-19 (WCPT, 2020 – see resources page)
Is there anyone who can benefit from IS?
Patients with recent rib fracture(s) until they can tolerate increased intensity of training. – Low Level Evidence
Pre-operative training for very deconditioned patients until more intense training is tolerated. – Moderate Level Evidence
So what the heck do I do with it?
Assessment of improvement of vital capacity when used before and after an intervention (i.e. PEP,IMT, diaphragmatic breathing) – Moderate Level
May help regulate the normal cough mechanism – Low Level Evidence
Follow @DoctorBthePT on Twitter for regular updates!
References:
Eltoria, A.E., Szabo, A.L., Antoci, V., Vantetuolo, C.E., Elias, J.A., Daniels, A.H., Hess, D.R. (2017). Clinical Effectiveness of Incentive Spirometry for the Prevention of Pulmonary Complications. Respiratory Care. 65(4). Retrieved from http://rc.rcjournal.com/content/early/2017/12/26/respcare.05679
Tyson, A.F., Kendig, C.E., Madebi, C. (2015). The Effect of Incentive Spirometry on Postoperative Pulmonary Function Following Laparotomy: A Randomized Clinical Trial. Jama Surgery. 150(3):229-236. doi:10.1001/jamasurg.2014.1846
Katsura, M., Kuriyama, A., Takeshima, T., Fukuhara, S., Furukawa, T. (2015) Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database of Systematic Reviews. http://doi.org//10/1002/14651858.CD010356.pub2
de Alvarenga, G. M., Remigio Gamba, H., Elisa Hellman, L., Ganzert Ferrari, V., & Michel de Macedo, R. (2016). Physiotherapy Intervention During Level I of Pulmonary Rehabilitation on Chronic Obstructive Pulmonary Disease: A Systematic Review. The open respiratory medicine journal, 10, 12–19. https://doi.org/10.2174/1874306401610010012
Ok, so homemade masks are THE THING right now. You will see that even I am wearing one in my “About” picture. My wonderful PTA Melissa made this one. It has a pocket on the inside in which we have placed HEPA filters cut from the vacuum bags this doctor recommends.
Some research will show that cotton masks are 3% effective, some will show that they may actually increase your chance of infection, and some people say, “Well, something is better than nothing.” And with actual surgical masks running low and N95s no where around, something may actually BE better than nothing! So what can you do to increase your chances of these actually working?
This emergency physician had a pretty good idea!
Forbes has issues the call to action for all who can sew to start sewing and making cotton masks for as many healthcare workers as possible.
Cotton masks can be sanitized by boiling in water for 20 minutes. This hasn’t damaged the elastic bands on any of my masks. Please do this as frequently as you can, daily at least. I have three masks that I rotate. The filters should be ok to go through the boil, but this may impact their filtration effectiveness.
Provides Positive Expiratory Pressure (PEP) to exhalation
Used for pulmonary hygiene to increase/maintain secretion mobility, increases sputum production
Promotes increased lung volumes due to re-inflation of collapsed airways
Changes focus to Exhalation instead of Inhalation!
Improves the efficacy of inhaled medications! See this post for more information!
Improves amount of time someone can participate in exercise and reduces the amount of time they need to recover dyspnea after exercise (see more about that here!).
You need to tell your patient that this will make them cough! That way, they don’t STOP using it because it made them cough! Getting them to cough is the whole point. They may not tolerate this will at first, so you may need to instruct them to spread out performance over the course of the day to increase tolerance.
Goal: maintain secretion mobility, produce cough, expel secretions
The Aerobika. Although useful and better than nothing, this device doesn’t function if turned upside down so using it in conjunction with postural drainage positions is challenging. However, it will still give the patient some resistance to exhalation with some oscillation to assist in loosening secretion as long as they are upright.
Duet Devices. Allow for all the benefits of a regular PEP device with the addition of the ability to run nebulizer medications through the device at the same time. Read more about that here! This is the standard, but there are other options.
Here is an article that outlines the very basics of different types of devices including PEPs, flutter valves, cough-assists, and more.
How do you like to combine your pulmonary interventions? Let me know in the comments!
If there is any treatment that I feel like gets used in a cookie-cutter fashion, it’s pursed-lip breathing. As much as I hate seeing this technique used for every single patient that has shortness of breath, it does have clinical usefulness. So let’s talk about how to implement pursed-lip breathing properly based on patient presentation…
We’ve all seen that dreaded picture in our textbooks… All the human figures laying in so many different positions with pillows and tables tilted all over… and I very clearly remember thinking, “How on earth am I supposed to remember all of those?” Well, good news. You really don’t have to. It’s great if you…
Olsen, et al. (2015) Respiratory Medicine Positive expiratory pressure – Common clinical applications and physiological effects. Resp Med: 109, 297-307;
Gastaldi AC (2016) Flutter Device Review: Effects on Secretion and Pulmonary Function. J Nov Physiother 6: 292. doi:10.4172/2165-7025.1000292.
We know the doctors, nurses, respiratory therapists, anesthetists, and all those other incredible people caring for patients in the ICU and ED are risking their lives every moment. But there is another side of this pandemic: the side that stays home.
Patients that stay home or are sent home still require care. Many may have comorbidities that require higher level skills (like pulmonary hygiene interventions or medication management) that can’t be performed virtually. So someone HAS to go to them instead.
The definition of “home bound” has completely changed. This is a term home health care providers are extremely familiar with. It is often a reason we have to deny services or discharge services: a patient has recovered to a point where they are no longer home bound. And most payers will NOT reimburse care provided in the home for those who are not home bound. However, due to the recent implementation of “shelter-in-place” orders across the country, EVERYONE IS HOME BOUND.
This means that the utilization of home health care based services will exponentially grow in accordance with the growth of COVID-19 cases. It is understandable. If you can’t go out because you are at high risk or you risk infecting others, then health care has to come to you. But what does that mean for the providers who go from house to house?
The number of health care workers who are infected climbs every day. Some are recovering, some are not. This isn’t meant to spread fear, it’s just the truth. We, as health care workers, are carriers just like everyone else if we have somehow been exposed.
Home care providers are at very high risk for infection due to the inability to maintain social distances from their patients, the manual interventions that require close contact, and the inability to ensure a clean and sanitary environment in which to practice. And that’s only the risk to us!
We also pose a significant risk to our patients! We go from house to house and are out in the world risking exposure and bringing it in with us. In to the homes of the MOST fragile, the homes of the very sick, and even group homes where we could infect many people at once.
But Physical Therapy is STILL a necessary service that many patients will require, not just to recover from COVID-19 or keep them of of ventilators, but to keep them out of the hospital for other conditions like vertigo, back pain, and injuries due to a fall.
If you are a home health care worker and you are feeling the strain of this, you are not alone. Many home health care therapists and other providers are sharing their concerns:
“….our profession plays a crucial role in the health of our society, and there are people in our communities whose health will be significantly impacted by disruptions to care.
[Physical Therapists should] use their professional judgment in the best interests of their patients and clients and their local communities – including rescheduling non urgent care if that is the best approach, or making other adjustments when the risk of exposure to COVID-19 outweighs the benefits of immediate treatment.”
So the question comes down to this: What care is truly necessary to be performed face-to-face? Are you implementing any virtual visit platforms to complete care that doesn’t have to be done face-to-face? How are you prioritizing your patient care?
If you are a home health care therapist, let me know what you think in the comments! Or share your tips with others!
Dr. Rebekah Griffith, other wise known as The ED PT, interviewed Dr. B on all things patient care management and how PTs in the ED and Home Health PTs can work together to provide the best possible care for patients. We talked about the struggles we each face in managing complex patients and the roles…
…to brush up on our respiratory intervention skills. These are my bread and butter. In the six years that I practiced in home healthcare, I learned to love these skills I never thought I’d need. And the more I grew to love them, the more I loved using them. But that means seeing the patients that are the most medically complex.
This brought me to heart and lung transplant care. That may seem scary for some people: providing aerobic exercise and respiratory interventions for patients who have just had their organs removed and replaced with someone else’s. But it is my passion. And that passion led me to get involved with the heart and lung transplant education team at my hospital system. I started providing the education courses for other PTs, OTs, and SLPs, so they could also provide these interventions and care for these patients with confident competence.
I can promise you, the patients being treated before or after transplant are just as scared as the ones being treated for COVID-19. No one knows what their outcomes will be. In lung transplant, we say “50% will live 5 years”. That may not sound like much, but many of these people are literally DAYS away from suffocating to death. It’s a chance they are willing to take.
With COVID-19, I imagine the feelings are the same. We don’t even know how long 50% of the hospitalized patients will live. We hope they return to the majority that recover, but not everyone will. Some will fall into that percentage that require extended hospitalization. The others will get the red tag.
I have taken a patient through YEARS of pulmonary pre-hab for a double lung transplant and many months of rehab after. She was on her way to visit family to say her final good-bye, trucking along her 10 L/min supply, when she got her phone call. The lungs were available. She knew what that meant, but she also knew she had to accept that reality quickly and get to the hospital. Thankfully, the family she was visiting lived nearby.
She had some rough road after her transplant, but it turned out to be successful. She had a beautiful two years of life after transplant. She returned to gardening, spending time outside, and welcomed a new grand-niece in to the world. So what kept her going?
SO. MUCH. PT.
Seriously, years of PT.
Obviously, you can’t do that in every setting. But, we spent our time strengthening her diaphragm using a Threshold IMT for progressive resistive exercise, diaphragmatic breathing activities with PNF-based manual inputs, practicing breathing with activity, PEP for airway clearance, active cycle of breathing, huffing, postural drainage, percussion, and even METs for rib mobility. She was in desperate need of cough efficiency planning because she had so little reserve.
I utilized auscultation and active pulse oximetry prior to and after interventions to demonstrate progress and instructed her in high-intensity interval training. Yes, even someone with advanced COPD, pulmonary hypertension, and an indwelling pulmonary catheter on 10 L/min of oxygen can do high-intensity interval training.
You can read more about this story here and see some beautiful pictures of respiratory interventions taking place. But more importantly, you can see the happiness that beams from her, even though she can hardly breathe.
If you’ve checked out the World Confederation of Physical Therapy’s Guidelines for PT Treatment of COVID-19 in Acute Care, you’ve seen these types of interventions listed. Patients who have COVID-19 need respiratory interventions from a skilled PT before they end up on a ventilator, during their ventilated time, and after they are removed from the ventilator. Active interventions should always be given priority over passive ones (aka EXERCISE!) but you do what you can. And don’t forget about contraindications for some interventions.
To perform these interventions properly for patients with COVID-19, the WCPT recommends that PTs who are already skilled and experienced in providing them be the ones to do so. However, that doesn’t mean you won’t see these patients outside of acute care. It’s time to brush up. It’s time to take back this part of our practice. We are the most skilled in providing physical interventions to improve cardiopulmonary function. If you haven’t done this stuff in a while, you can find online courses everywhere (or here!). We need more people providing these interventions because the demand is going to be high.
Image credit: Chris Clark, 2016
Do you think it’s time to brush up on your CV/P skills? Let me know what you feel like you need to most brushing up on in the comments!
Do you ever wonder, “did anyone else see that?” We find those red flags sometimes, don’t we? We see something odd in a physical exam and it completely changes our perspective on the patient. The key to seeing it, though, is to look for it. You may be thinking, “another thing I need to add…
Isn’t COVID-19 just a respiratory disease? If only that was true. We are good at treating respiratory infections. We have lots of drugs for viral, bacterial, parasitic, and fungal infections of the lungs. Most of them work really well! We also have several backup treatments, inhaled medications, and adjuvant therapies (like rehab!) that make primary…
Treating patients with acute and chronic clotting conditions is not new to rehabilitation professionals. We even have clinical practice guidelines around how to do so safely. However, what is new is the increased risk of newly acquired clotting conditions among post-COVID-19 patients. Those of us practicing in acute, subacute, emergency, and outpatient settings are uniquely tasked with…
I continue to receive numerous texts, emails, phone calls, and messages asking how the heck PTs are supposed to keep practicing amidst the trials of COVID-19. The laws are changing constantly, states are laying down practice restrictions, and payers are opening up and expanding, but amidst all that, many of us feel lost.
I’ve held leadership roles in our profession, but I definitely am no COVID-19 expert. What I can tell you is that Physical Therapists are incredibly strong, smart, undaunted, and resourceful. We have jumped at the chance to respond to pretty much every epidemic, pandemic, and natural disaster around the world since the inception of our profession. COVID-19 shouldn’t and won’t be any different.
Our sense of altruism is too strong. That’s why most of us are TERRIBLE at marketing ourselves. Our values are deeply engrained. That’s why we keep wondering how we can help.
I had the idea to start this site years ago, but the inundation of communication I’ve received related specifically to the current situation pushed me to open this up sooner than I had planned. I never imagined that I would be launching this site in response to a pandemic that has left my colleagues providing chauffeur services for other healthcare providers, or being a greeter at the front door of an urgent care, or applying to work at Costco. Yes, these are all things our fellow PTs are currently doing. And It’s killing me.
I, like Liam Neeson, have a very particular set of skills. I am a physical therapist who specializes in the management of advanced chronic disease. I do that by providing skilled interventions targeted at the cardiovascular, pulmonary, and neurological systems in the geriatric population. I spend most of my days treating end stage COPD, ESRD, or CHF, and I love it. As a PT, I want to see more people in our profession utilizing these types of skillsets. We all have them to some extent. We all learned this stuff somewhere along the way. I just kept learning it and never looked back. My goal is to help all of you relearn it, too. I want you to feel comfortable with the skillsets you will need to treat patients with advanced heart and lung diseases, like COVID-19. I want to teach what interventions you’ll need in your toolbox. Most of all, I want you to be able to keep doing your job because you are valuable and I want you to be able to prove it.
If you are an outpatient orthopedics therapist who doesn’t really remember much from cardiopulmonary class, this is for you. If you are a new grad who just wants to know everything you don’t know, this is for you. If you have been practicing in skilled nursing for 25 years and want an update, this is for you. If you don’t care at all about cardiopulmonary physical therapy services, but you know you need them right now, this is for you (but we should talk more later).
I want you all to feel confident in the competence you have in these skills. I want you to know that someone else is out there fighting for you and with you through all this crazy. I want you to know that there is somewhere you can go to brush up on all this stuff quickly and without cost so you can go right back to work tomorrow and DO these things. I want you to feel valuable and give value to your patients.
I hope you can find some help here. And once this passes, if it passes, I hope to re-focus on other practice issues.
Stay safe and stay healthy, because we can’t stay home.
This article can be read for free on MedBridge! Click the link below! Could the cardiotoxic effects of monocloncal antibody treatment be contributing to the ongoing effects experienced by those with long COVID? Let me know what you think in the comments!
I took a trip to Denver recently and, right around the same time, was consulted regarding the use of a pulse oximeter at high altitudes. It all got me thinking: how different could it really be to practice at 9,000ft? So, I did some work on this and I have to tell you, finding this…
I hope, at this point, you’ve all heard of the FAST acronym for identifying signs of a cerebrovascular accident (aka stroke). My in-laws even have a magnet on their fridge with a great comic strip describing the FAST acronym. I have run in to a couple different versions of it in the last few years,…
So, who’s up for some bloodwork? Venipuncture, anyone? Finger prick, maybe? No..? Oh… Well, ok then. I’ll carry on. I know it may sound a bit crazy, but as a PT, I actually do some (very) minor blood work. I’m not trained as a nurse or phlebotomist or anything like that. Nope. Just some on-the-job-training…
How many times have you had your temperature taken lately? I think I’ve had my temperature taken thousands of times in the last few months. We are seeing the increased use of forehead scanning thermometers and temporal scanners, all the non-contact forms of temperature assessment, to screen folks for COVID-19 symptoms upon entry to any…
I started this venture back in March in response to COVID-19. I saw many Physical Therapists and other rehab professionals shutting their doors because it wasn’t safe to keep them open. I saw an opportunity to improve our profession by addressing a deficit in practice: the lack of cardiopulmonary skill implementation. It wasn’t even that…
We finally have enough research and enough answers and enough patients and enough confirmed cases that have received care. We can start making some recommendations and have at least a minimal amount of evidence for some guidelines on treatment.
The World Confederation of Physical Therapy has published acute care guidelines for care of patients with COVID-19 specific to PTs. There are plenty of guidelines for physicians and nurses right now, most with a fiar amount of evidence, but not PT. We haven’t gotten much to guide us.
My favorite part of these guidelines is that it makes recommendations for who should and should NOT be seen for PT in a critical care setting. I feel like these recommendations for service triage will be modified for application to other settings. So many therapists are reaching out right now because they are struggling with the lack of definition of “essential” and this could be the answer. Some states (like Michigan) have taken it upon themselves to define “essential” as life-saving or life-sustaining care.
How do you feel your employers are doing with utilizing the term “essential” when it comes to patient triage? Take a look at these guidelines for triage and treatment.